Breast Cancer
Types, Treatment, and Survivorship Care
Online Continuing Education Course

Course Description
4-contact-hour breast cancer CEU on types, treatment, and survivorship care. This oncology continuing education course covers the care of patients with breast cancer, including types and diagnosis methods, current treatment modalities, survivorship, and end-of-life issues. Applicable for nursing, occupational therapy, and physical therapy. Bestseller!
Course Price: $30.00
Contact Hours: 4
Pharmacotherapeutic Hours: 1
Course updated on
February 2, 2023
"This was an excellent course. I even printed the PDF for future reference and review. The course effectively presented breast cancer components and treatments in a way that makes sense. I would definitely recommend this course to other oncology nurses to strengthen their current knowledge and to learn more in reference to basic knowledge." - Linda, RN in Ohio
"I have been a Breast Health Navigator for 12 years and am a CBCN through ONCC. I learned some new information with this course, and it was a great review. Very well done." - Kimberly, RN in North Carolina
"One of the most robust and comprehensive education opportunities on breast cancer that I have seen. Excellent course." - Eugenia, RN in Hawaii
"This course gave me a lot of new information I hadn't been aware of. A close friend was recently diagnosed with breast cancer, and this new knowledge will also help me understand processes she will be going though. A very thorough course." - Nancy, OTA in Kentucky








Breast Cancer
Types, Treatment, and Survivorship Care
Copyright © 2023 Wild Iris Medical Education, Inc. All Rights Reserved.
LEARNING OUTCOME AND OBJECTIVES: Upon completion of this course, you will be able to describe and summarize the considerations of care for people with breast cancer. Specific learning objectives to address potential knowledge gaps include:
- Review the types of breast cancer and its diagnosis and staging.
- Summarize the different treatments for breast cancer and their possible side effects.
- Discuss lifestyle management for individuals with breast cancer.
- Summarize the major components of survivorship care for breast cancer.
- Describe the implications and management of breast cancer recurrence.
TABLE OF CONTENTS
Breast cancer is the most common cancer among women in the United States and the second most common cause of cancer death in women (ACS, 2022b). Healthcare providers frequently manage women with breast cancer in the acute and chronic stages of the disease within a variety of clinical settings. This course will discuss the diagnosis/staging, treatment, and survivorship aspects of caring for patients with breast cancer.
UNDERSTANDING A BREAST CANCER DIAGNOSIS
The breast is made up of lobules (glands that produce milk), ducts (tiny tubes that carry milk from the lobules to the nipple), and stroma (connective and fatty tissue that surrounds the lobules and ducts, including blood and lymph vessels). Most of the lymph vessels in the breast lead to lymph nodes under the arm (axillary nodes).
Breast cancer normally arises in the epithelial cells that line the ducts and lobes of the breast, which are in constant turnover. These cells are generated continuously by a basal membrane and normally divide, migrate, and differentiate in a tightly controlled process. Cancer forms when internal (genetic alterations) or external (e.g., environmental and hormonal) factors interfere and the cells undergo an abnormal spectrum of changes, from hyperplasia to preinvasive to invasive and metastatic cancer.
The most common sign of breast cancer is a painless, hard lump with irregular edges. However, two thirds of lumps in the breast are not cancerous; they may be fluid-filled cysts, fibroadenomas (benign tumors), or pseudo lumps.
Warning signs of breast cancer may not be the same for everyone. Women should be aware of changes in the look and feel of their breasts as well as changes in the nipple or discharge from the nipple. Possible warning signs of breast cancer include:
- Lump, hard knot, or thickening inside the breast or underarm area
- Swelling, warmth, redness, or darkening of the breast
- Change in the size or shape of the breast
- Dimpling or puckering of the skin
- Itchy, scaly sore or rash on the nipple
- Pulling in of the nipple or other parts of the breast
- Nipple discharge that starts suddenly
- New pain in one spot that does not go away
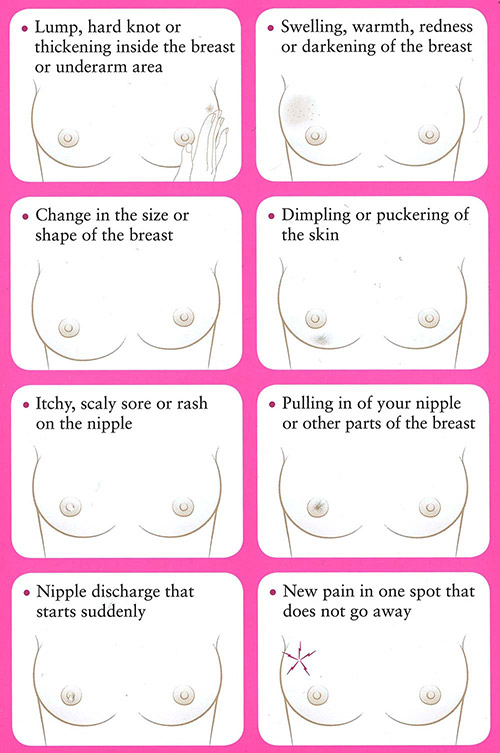
Warning signs of breast cancer. (© 2016, Susan G. Komen. Used with permission.)
Diagnostics
The process of diagnosing breast cancer may include a complete physical exam, assessment of risk factors, mammographic evaluation, other imaging tests, laboratory tests, and biopsy of the suspicious area. Biopsy is the most definitive step in the process, establishing whether the abnormality is benign (noncancerous) or malignant (cancerous) since no definitive diagnosis can be made without microscopic evaluation. If the diagnosis is breast cancer, the pathologist defines the type of cancer and whether it is invasive or noninvasive (in situ).
BIOPSIES
A biopsy involves removal of a small sample of tissue in the suspicious lesion for analysis in the laboratory. There are different types of biopsies, and each has advantages and disadvantages. Biopsies are performed by surgeons, radiologists, and/or pathologists and evaluated by cytopathologists (pathologists who specialize in cancer). Along with identifying cancerous cells, a biopsy can provide information about the type of cancer as well as hormone receptor status (ER, PR, and HER2), which is important in the process of treatment planning.
There are two categories of biopsies for breast tumors: needle biopsies and surgical (open) biopsies.
Needle biopsies are generally outpatient procedures and include:
- Fine-needle aspiration biopsy
- Ultrasound-directed needle biopsy
- Vacuum-assisted core biopsy
- Stereotactic core-needle biopsy
Surgical biopsies include:
- Needle-localization biopsy
- Excisional biopsy
IMAGING
Imaging tests are used to evaluate whether the breast cancer has metastasized (spread to any other parts of the body). This includes tissue surrounding the tumor, regional or distant lymph nodes, or other organs. The lungs are a common site for breast cancer metastases. Therefore, a chest X-ray is generally ordered during the diagnostic process. CT scans of the liver and brain are recommended only if metastases are suspected in those areas. Bone scans are done only if laboratory tests suggest the presence of bony metastases or if there are other known areas of metastases coupled with clinical presentation of bony pain. PET scans have proved more effective in detecting soft tissue metastases than metastatic bone lesions. However, the PET/CT combination is replacing CT in detecting soft tissue metastases because of its increased effectiveness (ACS, 2021c).
LABORATORY AND BIOMARKER TESTS
If a breast lesion is large and/or locally advanced—especially if any lymph nodes are involved—then the suspicion factor for distant metastases is raised, and they must be ruled out. The provider may order a number of blood tests to assess for signs of metastasis. For example:
- Serum alkaline phosphatase, which may signal liver or bone metastases
- Calcium levels, in which hypercalcemia may indicate bone metastases
Biomarkers are substances (i.e., hormone receptors or growth factors) that are present in cancer cells and help the cancer grow and spread. Testing for biomarkers can indicate specific characteristics of tumors that may help determine which treatment would be most effective in treating and preventing recurrence of the cancer.
The standard of care is to test breast tumors for hormone receptor status, including estrogen receptors (ER) and progesterone receptors (PR), along with human epidermal growth factor receptor 2 (HER2/neu) oncogene at the time of initial diagnosis (ACS, 2021a). This information is now used in staging breast cancer. Cancer treatments target these specific biomarkers by inhibiting the growth factors or blocking the hormone receptor to stop or slow the cancer growth.
Another important feature of the cancer pathology is the Ki67 expression. This marker is associated with cell proliferations and growth and has been shown to correlate with metastasis and the clinical stage of breast cancer (Brown et al., 2022). Knowing the Ki67 can help the physician understand how aggressive the cancer might be.
Types of Breast Cancer
Breast cancer is categorized based on pathology and the degree to which the cancer has spread. If the cancerous cells are confined to the ducts or lobules, the cancer is called noninvasive or in situ. Breast cancer that has spread through the walls of the ducts or lobules into the surrounding fatty and connective tissue is referred to as invasive or infiltrating.
INVASIVE DUCTAL CARCINOMA
Invasive ductal carcinoma accounts for about 80% of cases and is the most common form of breast cancer (ACS, 2021d). Originating in the ducts of the breast, invasive ductal carcinoma breaks through the wall of the duct into the breast tissue. It commonly forms a hard lump, which feels much firmer than a fibroadenoma (benign breast lump). On a mammogram, it usually appears as a mass edged with tiny spikes (spiculation).
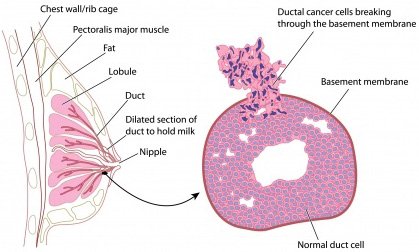
Cross section of breast with detail of ductal carcinoma. (Image © Peter Lamb; used with permission under license. May not be copied or downloaded without permission from 123RF Limited.)
INVASIVE LOBULAR CARCINOMA
Invasive lobular carcinoma is less common and originates in the lobules of the breast, where the milk is produced before it enters the ducts of the breast. It generally does not form a nodule or lump but spreads out and forms an area of thickening and fullness. Lobular carcinoma is also more difficult to see on a mammogram than ductal carcinoma. A number of research studies have linked invasive lobular breast cancer with use of hormone replacement therapy (Vinogradova et al., 2020).
TRIPLE-NEGATIVE BREAST CANCER
Treatment for breast cancer is often directed by characteristics of the cancer pathology (as discussed later in this course). People whose tumor pathology are estrogen receptor-negative, progesterone receptor-negative, and HER2/neu-negative are said to have triple-negative breast cancer. This is a rare subtype of breast cancer more common among younger people and those of African or Hispanic ancestry. It is highly aggressive, with distinct patterns of metastasis, and nonresponsive to hormone therapy or targeted therapy.
Brain and other visceral metastases are more common in triple-negative breast cancer than are bone metastases. Treatment for triple-negative breast cancer is usually surgery followed by traditional chemotherapy. Clinical trials continue to study new targeted therapies and immunotherapy for this type of cancer (CDC, 2021).
INFLAMMATORY CARCINOMA
Inflammatory breast cancer (IBC) is the most malignant form of breast cancer and accounts for about 1%–5% of all breast cancers in the United States. Some experts think IBC may be more common but underreported because it can be difficult to diagnose (ACS, 2022a). IBC is usually classified as stage 3B or stage 4, indicating that it has metastasized to distant sites at the time of diagnosis.
This aggressive subtype may be mistaken for an infection because it is characterized by swelling, pain, and reddened, warm skin over the breast. The inflamed appearance is caused by invasion of cancer cells into the subdermal lymphatic channels. If antibiotics do not rapidly change the appearance, biopsy is performed.
Standard treatment for IBC is chemotherapy to shrink the tumor, followed by surgery to remove the cancer. Radiation is given post surgery. Additional chemotherapy, hormone therapy, or targeted agents may also be recommended as treatment. This is especially true if IBC is advanced (ACS, 2022a).
Like triple-negative breast cancer, IBC is more common in young African Americans. It is also more commonly found in overweight or obese women.
Once a uniformly fatal disease with only an 18-month survival rate from time of diagnosis, IBC can now be treated more effectively. Recent data reports a 41% 5-year survival rate for IBC (ASCO, 2022a).
PAGET’S DISEASE OF THE BREAST
Paget’s carcinoma is a very rare cancer, accounting for only 1% of breast cancer cases. It primarily affects the nipple, presenting as itching or burning with superficial erosion or ulceration. In some cases, there is no breast mass. Like inflammatory breast cancer, Paget’s disease of the breast is often misdiagnosed, in this case as dermatitis, delaying proper diagnosis.
If cancerous changes are confined to the nipple, the prognosis is excellent. If a breast mass is present, the cancer may have spread to the axillary nodes or beyond. Treatment may include lumpectomy or simple mastectomy, depending on the extent of disease. Lumpectomy with removal of the nipple and areolar complex followed by radiation therapy is recommended to reduce the risk of recurrence (ACS, 2021f).
BREAST CANCER DURING PREGNANCY OR LACTATION
Breast cancer during pregnancy or breastfeeding is rare, but it can occur. Even though the tumor may be felt, both the patient and their primary care provider may mistake it for normal pregnancy-related changes in the breast, delaying diagnosis. This delay means that in two thirds of cases, the cancer has spread to the lymph nodes before it is discovered.
Depending on the stage of the pregnancy at the time of diagnosis, some patients may choose to terminate the pregnancy before beginning treatment. Others may choose to have a mastectomy during pregnancy and follow up with chemotherapy after the baby is born. However, studies have shown chemotherapy can be delivered safely during the second and third trimesters. Radiation treatment is not given during any stage of pregnancy due to the high risk of fetal harm.
Understandably, younger patients who have not started or completed their families may be concerned about their subsequent fertility, as well as increased mortality by becoming pregnant after breast cancer. Most research so far has shown that pregnancy is possible and safe for both the fetus and the mother after early breast cancer treatment in young women without increasing the risk of recurrence. It is important for patients to discuss fertility prior to treatment in order to plan for best outcomes.
Staging
Staging describes the extent of cancer in the body. The primary elements are based on whether the cancer is invasive or noninvasive, the size of the tumor (T), lymph node involvement (N), and metastasis (M) to other parts of the body. The stage of a cancer (on a scale of 1 to 4, with 4 being the most advanced) describes how advanced the disease is and helps determine the course of treatment. Many breast cancers today are detected at stage 1 or 2. In situ cancer, usually ductal carcinoma in situ (DCIS), is called Stage 0. Within a stage, an earlier letter (a) means a lower stage within that number.
The most widely used staging system for breast cancer—the American Joint Committee on Cancer (AJCC) TNM system—was updated in 2018 to include seven key pieces of information. (These are also referred to as the pathologic prognostic stage group.) The treatment team uses AJCC staging to evaluate the stage of the disease and plan appropriate treatment. This is now quite complex and takes into account many individual factors (ACS 2021a; Giuliano et al., 2018).
AJCC staging includes the following elements to formally stage breast cancer:
- Size of the tumor (T)
- Spread to nearby lymph nodes (N)
- Spread (metastasis) to distant sites in the body (M)
- Estrogen receptor (ER) status
- Progesterone receptor (PR) status
- HER2/neu (HER2) status
- Grade of the cancer (G), based on how normal or abnormal the cells appear when examined microscopically
TREATMENT OF BREAST CANCER
For many years, breast cancer was assumed to be a localized disease, and the treatment of choice was also localized: a radical mastectomy. However, when it was shown that these often disfiguring and debilitating surgeries were not improving survival or decreasing recurrence rates, this practice was abandoned.
As technology gets ever more sophisticated at detecting cancer cells, the view of breast cancer as a systemic disease gains more support. Thus, treatment of breast cancer today generally includes some combination of localized (surgery and radiation therapy) and systemic treatments (chemotherapy, hormonal therapy, targeted biological therapies, or immunotherapy).
Surgery is often the primary treatment for breast cancer, followed by radiation therapy. Depending on a number of factors, chemotherapy and/or hormone therapy may also be administered over weeks or months. The medical oncologist may recommend one or more of these therapies, depending on the patient’s age and the stage and other characteristics of the tumor. The goal of systemic treatment is to destroy any cancer cells that have moved beyond the breast to other areas of the body and to achieve long-term remission of the cancer.
Medical scientists previously thought that a tumor had to reach a certain size before cancer cells moved into the bloodstream and traveled to other parts of the body. However, research has shown that cancer cells can migrate out of the breast very early in the development of a tumor. This is why systemic therapies (chemotherapy, biological therapy, immunotherapy, and/or hormone therapy) are recommended for premenopausal women with breast cancer even if there is no evidence of cancer in the lymph nodes.
Radiation therapy, chemotherapy, hormone therapy, and targeted biological therapy are referred to as adjuvant therapy, or therapies given after surgical intervention. However, there are situations when the sequencing of surgery and the administration of systemic therapies may need to be modified.
Some practitioners prefer to administer chemotherapy and/or hormone therapy before surgery to remove the tumor, which is called neoadjuvant therapy. Neoadjuvant therapy may shrink large tumors, thereby enabling patients to have a lumpectomy rather than a mastectomy. It also enables the oncologist to evaluate a drug’s effectiveness in an individual patient.
Timing of neoadjuvant therapy also has implications for lymph node assessment (see below). Current practice is to perform sentinel lymph node biopsy (SLNB) before systemic therapies (ACS, 2021d). If no cancer cells are found in the sentinel node(s), the patient can avoid axillary lymph node dissection and avoid radiation to the axilla. This can reduce the risk of lymphedema, a painful, disfiguring, chronic swelling that can affect the entire arm and hand.
Surgical Interventions
Surgery is a cornerstone of treatment for breast cancer. Whether it precedes or follows systemic therapy, however, depends on a number of factors, including the stage of the cancer, the age of the patient, and the preferences of the treatment team. Patients with breast cancer may have a lumpectomy or one of three types of mastectomy (surgery to remove the breast).
Depending on the patient’s age, general health, and the size, type, and stage of the tumor, they may need only surgery and perhaps radiation therapy. But many patients, especially those who have not reached menopause, may need to consider adjuvant systemic therapy: chemotherapy, hormonal therapy, or targeted biological therapy (NCCN, 2022a).
LUMPECTOMY
Also called segmental mastectomy or wide local excision (WLE), lumpectomy is the removal of the tumor and a narrow margin of the surrounding tissue. The margin is taken to increase the chance that all of the cancer cells are removed. This type of surgery allows as much of the breast tissue as possible to remain. Because tumors are now detected at an earlier stage and often are smaller in size, lumpectomy is a common procedure.
Lumpectomy may not produce a good cosmetic result for a patient who has a large tumor in a small breast. However, large tumors sometimes can be reduced prior to surgery either by neoadjuvant chemotherapy, endocrine therapy, or biologic therapy (e.g., HER2-directed), making lumpectomy a viable option. These neoadjuvant therapies also show whether the tumor is responding to a specific therapy.
Current options for treatment include lumpectomy followed by a course of radiation therapy to destroy any remaining cancer cells that could cause recurrence or metastasis. Additional options may include accelerated (hypofractionated) partial breast irradiation and proton beam radiation (see also below under “Types of Radiation”). Radiation therapy reduces the locoregional recurrence rate and risk of breast cancer death.
Some patients, particularly older patients with very small, slow-growing tumors (<1 cm), may choose not to have radiation therapy (NCCN, 2022a).
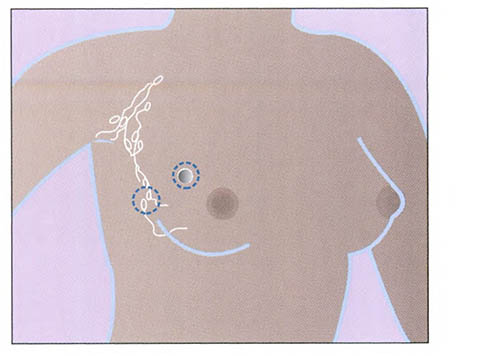
Lumpectomy. (Source: National Institutes of Health.)
MASTECTOMY
Mastectomy is a general term for removal of the breast. A mastectomy may be performed when a lumpectomy is not possible or based on the preference of the patient. There are three types of mastectomy: simple, modified radical, and radical.
- A simple mastectomy involves the removal of the breast tissue, skin, areola, and nipple, but not the lymph nodes. This procedure is generally used when axillary lymph nodes do not need to be removed, as evidenced by a negative sentinel node examination.
- A modified radical mastectomy involves the removal of the entire breast, including the skin, areola, and nipple, along with the axillary lymph nodes, but leaves the chest wall muscles intact.
- A radical mastectomy involves removal of the entire affected breast, the underlying chest muscles, the lymph nodes under the arm (axillary node dissection), along with some additional fat and skin. Radical mastectomies are rarely used today. This type of mastectomy is generally limited to cases when cancer has spread to the chest wall muscles.
Some patients with cancer in one breast may choose to have the other breast removed at the time of their mastectomy. This is called a bilateral mastectomy, and removal of the other breast is considered a prophylactic (preventive) measure. Prophylactic mastectomy reduces the risk of breast cancer developing in the contralateral breast, but it is not an absolute guarantee because of the systemic nature of the disease.
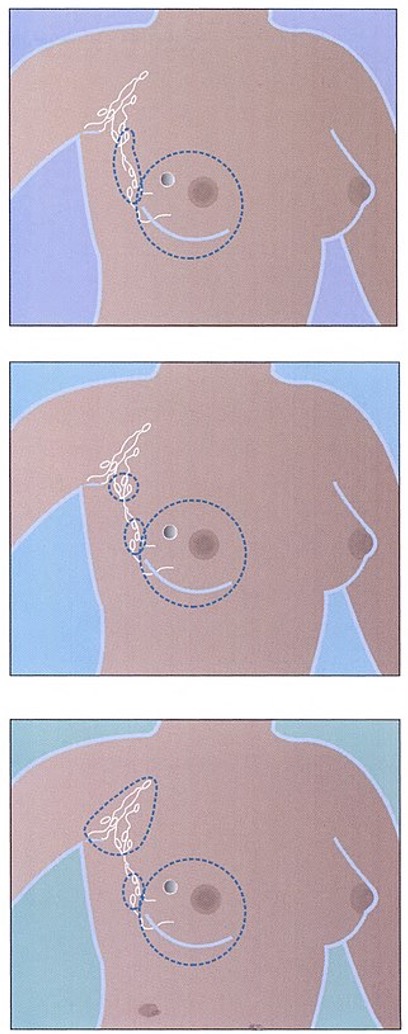
Total (or simple) mastectomy (top), modified radical mastectomy (middle), and radical mastectomy (bottom). (Source: National Institutes of Health.)
PHYSICAL THERAPY AND BREAST CANCER SURGERY
A physical therapist may work with a breast cancer patient before surgery as part of a prehabilitation plan. Prehabilitation is the period of time after diagnosis and before treatment starts. Many patients have a few weeks during this time to start assessments and learn the important steps to take to prevent complications such as lymphedema.
The goals of physical therapy during prehabilitation are:
- Take baseline measurements, such as the circumference of both arms and range of motion (ROM) of shoulder movements
- Identify any individual concerns that may affect recovery, such as muscle weakness, deconditioning, and pain syndromes
- Educate the patient and family on lymphedema and how to prevent complications
- Establish a personalized exercise program for before and after surgery
After surgery, the goals of physical therapy are to minimize side effects of treatment and improve function. This may include:
- Manual therapy: Hands-on treatment to the joints, muscles, and incision areas aimed at reducing range of motion problems, cording, scar formation, and pain and swelling
- Lymphedema treatment: Assisting with manual lymphatic drainage, compression bandaging, assessment for garments, and exercise instruction
- Exercise plan: Continued support with an individualized exercise plan during and after treatment (and into the survivorship period) to reduce side effects such as fatigue, pain, and lymphedema
(Koesters, 2021)
LYMPH NODE ASSESSMENT AND REMOVAL
Lymph nodes are part of the immune system and linked by tiny vessels within the entire lymphatic system. Lymph nodes and the lymph vessels drain the excess fluid that is not absorbed by blood vessels. Lymph nodes filter out foreign substances such as bacteria and cancer cells as part of the body’s immune system.
In addition to performing breast surgery, surgeons examine underarm lymph nodes for cancer cells using either an axillary lymph node dissection or sentinel lymph node biopsy. Lymph node assessment is performed for two reasons: 1) to determine whether the cancer has spread beyond the breast, and 2) to remove any cancerous nodes. Oncologists use this information in staging the tumor and as a basis for planning optimal treatment (ACS, 2021d).
Axillary lymph node dissection (ALND) involves removal of a large number of axillary lymph nodes for examination by a pathologist. Formerly a part of all breast cancer surgeries, axillary dissection has been replaced in many cases by a newer procedure called sentinel lymph node biopsy.
Sentinel lymph node biopsy (SLNB) is also called sentinel lymph node dissection. This newer procedure offers a less-traumatic alternative for determining whether the cancer has spread beyond the breast. The SLNB procedure focuses on locating the specific lymph nodes (sentinel nodes) that are first to receive drainage from the breast tumor.
SLNB is most appropriate for patients with early-stage breast cancer with clinically negative axillary nodes. For patients who have axillary nodes identified positive for cancer cells with the SLNB, ALND completion is performed. Physical examination, imaging studies, and tumor size help determine the most appropriate type of lymph node sampling.
SLNB results in fewer complications and less lymphedema than ALND. The procedure is usually done at the same time as either lumpectomy or mastectomy. Before the tumor is removed, a radioactive substance is injected into the area surrounding the tumor. About an hour later, in the operating room, the surgeon injects a special dye near the tumor and makes a small incision in the underarm area. By tracking the path of the dye and the radioactive substance, the surgeon can identify and remove the sentinel node (or up to three nodes) where cancer cells from a breast tumor would reach first.
The node(s) are sent to the pathology laboratory for examination while the patient is still in surgery. If no cancer cells are found in the sentinel node(s), no further nodes are removed—only the tumor itself. If cancer cells are found, however, the remaining nodes are removed and analyzed using standard axillary dissection technique (NCI, 2022).
LYMPHEDEMA AS A SIDE EFFECT OF SURGERY
Lymphedema is the interstitial collection of protein-rich fluid due to disruption of lymphatic flow. It is a common complication of axillary node dissection and radiation therapy. Breast cancer treatment is the leading cause of secondary lymphedema.
When the patient has an axillary surgery or a SLNB and radiation, the risk of lymphedema increases. Most patients who develop lymphedema will do so within three years of surgery, but it is important that patients understand it remains a lifetime risk.
Signs and symptoms of lymphedema include:
- Fullness, aching, pain, or heaviness in the arm
- Feeling of tightness of the skin of the arm and hands
- Reduced range of motion of the affected arm
- Clothing or rings that no longer fit on the affected side
(Manahan, 2022)
Diagnosis and evaluation of lymphedema is done with imaging of the lymphatic system called lymphoscintigraphy (radionuclide imaging). This type of imaging may be performed on patients at high risk for lymphedema. MRI imaging may also be added to gain additional information about the extent of lymphedema and nodal involvement.
The risk and extent of developing lymphedema depend on whether and how many lymph nodes are removed and whether or not radiation treatment is added to surgery.
It is critical to recognize lymphedema at the earliest possible stage to educate the patient and initiate treatment to prevent worsening of the condition. The table below describes the stages of lymphedema based on severity.
| Stage | Type |
|---|---|
| (ACS, 2021h) | |
| 0 | No swelling, but subtle symptoms such as feeling the affected area is heavy or full or that the skin is tight |
| 1 | Swelling of the affected area, increased size or stiffness of the arm; swelling that improves when the affected arm is raised |
| 2 | More swelling than stage 1, which does not improve when the arm is elevated; arm hard and larger than in stage 1 |
| 3 | Much more swelling than stage 2, possibly so severe that the patient cannot lift or move the arm on their own without using their other arm; dry and thick skin; fluid leaking from the skin or blisters forming |
Risk of lymphedema is lifelong after breast cancer surgery or radiation therapy, especially when axillary lymph nodes are involved. Therefore, patients must reduce risks of developing the disorder through precautionary measures such as:
- Controlling one’s weight
- Avoiding arm constriction (no restrictive clothing or blood pressure cuffs on the affected side)
- Avoiding punctures (no injections, IVs, blood draws, or acupuncture on the affected side)
- Using compression garments as appropriate
- Avoiding extreme temperatures, such as with hot tubs
- Keeping the arm clean and dry; applying moisturizer daily
- Avoiding resting the arm below the heart or sleeping on the affected arm
- Wearing gloves when gardening or using household cleaners
- Avoiding carrying heavy over-the-shoulder bags or purses on the affected side
- Monitoring for signs and symptoms of infection (fever, swelling, redness, pain, and heat) and seeing a physician for evaluation immediately
(ACS, 2021g)
It is imperative that nurses and healthcare providers instruct patients on the above symptoms to report and precautionary measures to take both before and after surgery as well as reviewing this during treatments and follow-up appointments.
While there is no cure, treatment for lymphedema is available and is best started at the first sign of swelling. Healthcare providers and rehabilitation specialists can work with patients before surgery to focus on prehabilitation when possible and must be vigilant in assessing patients for any problems after surgery during follow-up appointments. Assessment may include asking questions about symptoms, quality of life, and activities; taking measurements on the affected arm; skin inspection; and palpation.
The goal of treatment is to decrease the swelling as much as possible and maintain the limb at its smallest size. This helps prevent or eliminate infections and minimize discomfort. Treatments include complete decongestive therapy, manual lymph drainage, and compression, as prescribed by a physical therapist, occupational therapist, or other certified lymphedema specialist.
Patients with post-treatment edema or early signs of lymphedema are referred to a lymphedema specialist to initiate evaluation and instruction on complete decongestive therapy, which includes four components:
- Manual lymphatic drainage. This is a specific massage technique that uses gentle and progressively directed manual (by hand) massage, following the direction of the natural flow of lymph. It is generally shown to produce excellent results.
- Compression bandaging techniques or wearing of compression garments. Compression bandages or garments are customized to the individual patient and can provide the specific level of support needed to reduce edema. Bandages or garments can be used on a regular basis to help keep swelling and symptoms under good control.
- Exercises to promote lymph drainage. Patients are taught by rehabilitation specialists to perform regular and specific exercises of the shoulder joint, as well as at the elbow, wrist, and hand.
- Skin care. Patients are instructed to keep their skin clean, dry, and hydrated with a gentle moisturizer. Daily inspection for any edema is encouraged. Patients are instructed to report any new swelling, heaviness, or pain to their healthcare provider right away, even if it has been a long period of time since treatment was completed.
(MSKCC, 2022)
OCCUPATIONAL THERAPY AND LYMPHEDEMA
Occupational therapy services are an integral part of managing lymphedema treatment. Occupational therapists (OTs) require additional training to become lymphedema certified (CLT-LANA). Once certified, OTs may include the following interventions:
- Conducting baseline assessments and preoperative education on what to watch for and how to prevent postoperative lymphedema
- Ongoing screening and monitoring for any problems
- Education and training on postoperative therapeutic range-of-motion exercises as well as incorporating activities of daily living such as grooming and bathing
- Providing information on how to prevent lymphedema by modifying lifestyle habits and clothing and assessing occupational risks
- Providing treatment with manual lymph therapy
- Referring patients to other support programs
- Providing education on self-care management, including skin care, infection prevention, compression garments, and adaptive clothing
(AOTA, 2021)
RECONSTRUCTIVE SURGERY
Breast reconstruction is a surgical procedure performed by a plastic surgeon and may require a longer recovery than mastectomy alone. Reconstruction can be performed at the same time as a mastectomy (immediate reconstruction), or it can be done later (delayed reconstruction). Immediate reconstruction may not be possible if the tumor is advanced and radiation is recommended. With immediate reconstruction, chemotherapy treatments are usually delayed for at least two to three weeks after surgery.
Breast reconstruction may be contraindicated for women who have diabetes, smoke, are obese or very thin, or have blood circulation problems.
There are options available with reconstructive surgery, but they are not all appropriate for every candidate. Essentially, there are two categories:
- Implant-based: Reconstruction using a tissue expander inserted into the affected area of breast, which is then injected with saline over a period of months and later replaced with a silicone or saline-filled silicone implant
- Autologous tissue: Reconstruction using the patient’s own tissue (most commonly transferred from the abdomen or the buttocks) to create a new breast mound
(NCI, 2022)
Radiation Therapy
Radiation therapy uses high-energy particles or rays, which produce at least three main effects:
- Inducing apoptosis, or programmed cell death, by invoking the preexisting signaling cascade through radiation damage, which results in cell self-destruct
- Causing permanent cell-cycle arrest or terminal differentiation (i.e., blocking cancer cells from moving beyond a cell cycle, rendering them unable to proliferate)
- Inducing cells to die as they attempt cell division (i.e., damaging the DNA, which results in an unsuccessful mitotic phase and causes cell death)
There are several reasons radiation therapy is utilized in treating breast cancer:
- After breast-conserving surgery (BCS), to decrease local recurrence rate
- To reduce the risk of recurrence after mastectomy when:
- The breast tumor is >5 cm
- Axillary lymph nodes test positive for cancer cells
- Margins of the tumor site are narrow and test positive for cancer cells
- In recurrent disease, to control metastasis
- To palliate symptoms of metastatic disease
(NCCN, 2022a)
TYPES OF RADIATION THERAPY
The most common way radiation therapy (RT) is delivered in breast cancer patients is through external beam radiation. RT can be delivered in various schedules. A common schedule has been to deliver external beam radiation therapy once per day, five days per week, for five to six weeks starting approximately one month after surgery. If a patient is also receiving chemotherapy, radiation therapy is typically started three to four weeks after completion of therapy (ACS, 2021g).
The daily schedule can present a challenge for patients, especially if they have to travel a distance to reach an RT facility. Travel expense, transportation, employment issues, and even childcare can all contribute to difficulty in complying with the RT schedule. Scheduling radiation appointments early in the day or at the same time each day often assists patients with their work/life schedules. Many patients continue to work throughout radiation therapy. For patients with such concerns, a social worker can assist in developing the plan of care, encouraging the patient to seek assistance from friends and family and referring to local support groups.
Newer approaches such as hypofractionated radiation therapy (also called accelerated breast irradiation) administer larger doses over a shorter time span (three weeks versus five to six weeks) for patients with negative lymph nodes after BCS. The hypofractionated radiation schedule appears to be just as effective as standard therapy in preventing recurrence and is more convenient for patients (ACS, 2021g).
Another newer approach called 3D-conformal radiation therapy is given with special machines that deliver radiation to the localized area where the tumor was removed (tumor bed). This allows treatment to a targeted area with less damage to healthy tissue. Treatments are given twice a day for five days. This is considered to be accelerated partial breast irradiation (ASC, 2021g).
External beam radiation can also be given intraoperatively at the time a lumpectomy is performed on early-stage breast cancer. In this approach, a single, large dose of radiation is directed at the lumpectomy site before the incision is closed (ASC, 2021g).
In proton beam therapy, a particle accelerator generates a highly charged beam consisting of positively charged protons. The approximately 5-millimeter beam can be finely controlled in its width, height, and depth so that it is directed specifically within the three-dimensional contours of a breast tumor. Proton beam is being investigated as an adjuvant radiation therapy for early and locally advanced stages of breast cancer. While the role of proton beam is still being discovered, rapid technological advances are poised to improve outcomes for patients with breast cancer (Mutter et al., 2021).
Another form of radiation therapy is internal radiation, or brachytherapy. Brachytherapy uses radioactive pellets, seeds, wires, or catheters that are temporarily placed in the breast tissue adjacent to the cancerous area or in the space where the tumor was removed. This method is often used in conjunction with external beam RT to give an extra “boost” in patients after BCS.
Brachytherapy targets radiation only to the area of the breast around the location of the tumor prior to surgery (generally, the lumpectomy cavity, plus 1 to 2 centimeters beyond the surgical edge). Brachytherapy is given over a period of four to five days and minimizes radiation exposure to other parts of the body. The rationale behind breast brachytherapy is to intensify treatment to the area most at risk for recurrence. Brachytherapy has fewer side effects, better cosmetic results, and improved overall quality of life during the treatment period (ASC, 2021g).
SIDE EFFECTS AND LATE EFFECTS OF RADIATION THERAPY
Both short- and long-term side effects are possible with radiation treatment. The two most common short-term side effects are fatigue and skin reactions in the irradiated area. In most cases, neither effect is noticeable until at least halfway through the six weeks of treatment.
Fatigue is the most common side effect in women undergoing radiation treatment and may last for several weeks or months after treatment. The level and length of the fatigue is as varied as the individuals experiencing it. Patients are taught to anticipate some level of fatigue along with various strategies to conserve energy.
Skin reactions to radiation can range from a mild “sunburn” effect to severe rash and swelling. Patients are taught to protect the radiated skin from exposure to harsh soaps and lotions, to avoid sun exposure, and to protect their skin from extreme temperatures (such as a hot bath or hot shower). Other skin-related side effects may include skin irritation, soreness, peeling, blistering, and decreased sensation or hypersensation (NCI, 2021). Healthcare providers may prescribe or recommend topical ointments and medicated creams to help treat skin damage.
Patient self-care strategies for skin care include:
- Wash the radiated area gently with warm (not hot) water and a mild soap.
- Do not shower more than once per day; limit baths to twice weekly for less than 30 minutes per bath.
- Avoid rubbing, scrubbing, or scratching the skin.
- Be careful not to wash off the ink markings needed for radiation therapy.
- Wash off any lotions or creams from sites prior to RT, as their presence can intensify burns.
- Gently pat skin dry after bathing.
- Avoid deodorant or talcum powder on the radiated side.
- Wear soft clothes and use cotton sheets.
- Avoid adhesive tape, bandages, or other types of sticky tape on the treatment area.
- Avoid chlorinated swimming pools and hot tubs during radiation treatment.
- Always protect the radiated area from exposure to the sun or tanning beds, even after treatment ends.
- Promptly report pain, swelling, exudate, or other skin changes to one’s primary care provider.
More serious (uncommon) side effects include swelling in the arm, lung damage, nerve damage, heart damage, and increased chance of rib fracture (NCI, 2021).
There is a slight risk of developing pneumonitis (a transient lung inflammation) following chest-wall irradiation. The risk can be greater depending on the exact field that is radiated. Patients undergoing RT are instructed to report a persistent dry cough, shortness of breath on exertion, the inability to take a full breath, chest pain, fever, malaise, or weight loss. Lung problems can occur anywhere from four weeks to 12 months after treatment.
Other short-term side effects of internal radiation include redness, bruising, breast pain, infection, weakness, rib fracture, and breakdown of fat tissue in the breast (NCI, 2021).
Radiation therapy can also have serious long-term complications. As mentioned earlier, radiation therapy increases the risk of lymphedema, which is chronic and can appear even years after treatment.
Radiation therapy for breast cancer can also slightly increase the risk of secondary malignancies, including leukemia, lung cancer, a small risk of contralateral second breast cancer, esophageal cancer, or a rare type of cancer called angiosarcoma. These cancers may develop 10 or more years after treatment in the tissue that has been radiated (ACS, 2022b).
Systemic Therapies
Treatments for breast cancer also include systemic therapies, which use the body’s circulatory and lymphatic systems to deliver therapies directly to the site of disease at a cellular level. Systemic therapies can be used in the neoadjuvant and adjuvant settings or to treat cancer that has metastasized outside the original tumor site.
Systemic therapies include endocrine therapy, chemotherapy, targeted therapies, biologics, and/or a combination of therapies.
ENDOCRINE THERAPY
Decades of research indicate that the hormone estrogen is linked to the development of a certain type of breast cancer and to the likelihood of its recurrence. That is why in the past, surgical removal of the ovaries (oophorectomy) often caused breast cancers to regress, and oophorectomy is still offered to estrogen receptor–positive (ER-positive) patients with extensive disease.
Today, however, the primary long-term treatment for ER-positive breast cancer is the use of drugs that interfere with the production of estrogen, which reduces the chance of recurrence or metastasis of ER-positive breast cancer. Two groups of drugs that affect estrogen production in the body are selective estrogen response modulators (SERMs) and aromatase inhibitors.
Options for premenopausal patients who are ER-positive include treatment with SERMs, ovarian ablation, or a combination of ovarian suppression in combination with SERMs. Aromatase inhibitors are also recommended for premenopausal women with metastatic ER/PR-positive breast cancer (after medical or surgical menopause) (NCCN, 2022a).
Selective Estrogen Receptor Modifiers
Selective estrogen receptor modulators include tamoxifen, raloxifene, and toremifene. SERMs stop estrogen from stimulating breast cancer cell growth by blocking the estrogen receptors.
Tamoxifen (Nolvadex) is the mainstay of hormone therapy for breast cancer and can be used in many ways, including:
- To treat women with invasive or noninvasive ER-positive breast cancer. Tamoxifen is used along with surgery to reduce the chance of recurrence. It can also reduce the risk of cancer in the opposite breast. Tamoxifen can be given either as neoadjuvant therapy or adjuvant therapy and is usually taken for five to ten years. For early-stage breast cancer, this drug is mainly used for women who have not yet gone through menopause.
- To treat women with advanced-stage ER-positive breast cancer. Tamoxifen can help slow or stop cancer growth and shrink tumors.
- To treat women who are at a higher risk for breast cancer. Tamoxifen can be used as a preventive medicine to lower the risk of developing breast cancer.
Unlike chemotherapy, tamoxifen does not cause neuropathy or mucositis, but it does have side effects that can alter quality of life and even be life threatening. The most common side effects are hot flashes, vaginitis, nonbloody vaginal discharge, induced menopause, sexual dysfunction, depression, and mood swings. While rare, in some patients tamoxifen can hasten the development of cataracts or cause fractures, blood clots in the lungs or legs, stroke, and/or endometrial (uterine) cancer.
Depending on the age of the patient and tumor characteristics, the oncologist may recommend chemotherapy and/or radiation therapy as well as tamoxifen. The preferred sequencing for tamoxifen is initiation of the medication after chemotherapy is complete (NCCN, 2022a).
Raloxifene (Evista) is a newer drug than tamoxifen. It was approved in 1997 to prevent osteoporosis after menopause. However, early studies of raloxifene also suggested that the drug reduced the risk of breast cancer without the risk of uterine cancer that tamoxifen carries, but with a similar risk of blood clots. Subsequent studies confirmed these findings, so raloxifene is sometimes prescribed to reduce the risk of breast cancer in women who do not have breast cancer but are at high risk for developing the disease and who are postmenopausal with an intact uterus.
Toremifene (Fareston) is indicated in the treatment of metastatic breast cancer in postmenopausal women with either ER-positive or unknown status. It is not likely to work well if tamoxifen has been used and stopped working.
Selective Estrogen Receptor Degraders (SERDs)
SERDs block and damage estrogen receptors with an anti-estrogen effect in the entire body.
Goseraline acetate (Zoladex) is used in pre- or perimenopausal women with ER-positive advanced disease to induce menopause. It is injected into the subcutaneous abdominal tissue either every 28 days or every three months if given in the depot form. Adherence to the treatment schedule is important with Zoladex, especially in the nondepot form. Long-term use may cause osteoporosis.
Fulvestrant (Faslodex) is indicated for postmenopausal women with metastatic ER-positive breast cancer that has failed first-line, anti-estrogen therapy. It is administered as an intramuscular (IM) injection once monthly and comes in a prefilled syringe.
Newer oral SERDs are also being developed. Elacestrant (Orserdu) gained FDA approval in 2023 for postmenopausal women or adult men with ER-positive, HER2-negative, ESR1-mutated advanced or metastatic breast cancer who have undergone at least one line of endocrine therapy. Elacestrant is an oral pill taken daily until no longer tolerated or disease progression.
Aromatase Inhibitors (AIs)
Aromatase is an enzyme produced in body fat and other tissue, particularly the breast. After menopause, when the ovaries no longer produce estrogen, aromatase converts hormones called androgens, produced by the adrenal glands, into estrogen. This conversion serves as the body’s main source of estrogen after menopause and therefore raises the risk of breast cancer and recurrence. For this reason, it is thought that excess body fat in postmenopausal women may increase the risk of breast cancer (ACS, 2021i).
AIs inhibit (block) the conversion of androgens to estrogens, thereby limiting the amount of estrogen that can reach cancer cells. This can lead to regression or stabilization of a tumor. However, AIs also act on other estrogen-sensitive tissues, which may account for some of the drugs’ side effects, such as muscle and joint pain and bone loss. Bone loss can increase fractures of the hip, spine, or wrist (ACS, 2021b). Additional side effects of AIs include hot flashes, vaginal dryness, and vaginal atrophy.
While tamoxifen is still an option for adjuvant endocrine treatment in postmenopausal women, AIs have been found to be more effective in preventing cancer recurrence in the first two years following breast cancer surgery. Aromatase inhibitors are not associated with the thromboembolic events and uterine cancers that are seen with tamoxifen (ACS, 2021b).
Currently, it is recommended that patients with ER/PR-positive breast cancer take an AI for at least five years. For those who do not tolerate or for other reasons do not want to take an AI, tamoxifen for at least five years is recommended (ACS, 2021b).
Three aromatase inhibitors have been approved by the FDA for use in advanced cancer: anastrozole (Arimidex), letrozole (Femara), and exemestane (Aromasin). Anastrozole has also been approved as adjuvant therapy for postmenopausal women with hormone-responsive-positive breast cancer. This is an oral therapy taken daily. Aromatase inhibitors can increase the risk of osteoporosis; therefore, it is recommended that women have a dual energy X-ray absorptiometry (DEXA) scan when treatment is initiated and continuing every two years to evaluate bone density (ACS, 2021b).
PREVENTING AND TREATING AI-INDUCED BONE LOSS
Zolendronic acid (Zometa), a bisphosphonate, and denosumab (Xgeva, Prolia), a monoclonal antibody, are both approved drugs used to prevent and/or decrease AI-induced osteoporosis and risk for bone loss in breast cancer patients.
Bisphosphonates work by inhibiting resorption of bone by osteoclasts and have been studied extensively in breast cancer patients. These drugs have also been shown to decrease risk of bone metastasis and may increase overall survival. Bisphosphonates are generally administered intravenously every six months for three years, for a total of six doses. Occasionally, bisphosphonates are administered orally to patients who have or develop osteoporosis.
Denosumab is a human monoclonal antibody that targets the RANK ligand (RANKL) protein, which acts as the primary signal promoting bone removal. By inhibiting the development and activity of osteoclasts, denosumab decreases bone resorption and increases bone density. Denosumab is also given every six months for three years (Eisen, 2022). Denosumab cannot be stopped without starting bisphosphonates, as there is a risk for rebound fractures.
Vitamin D and calcium supplementation may also be indicated in patients treated for breast cancer to aid with bone mineral density.
CHEMOTHERAPY
Administration of chemotherapy generally occurs after surgery for breast cancer; this is called adjuvant chemotherapy. However, patients with large tumors may receive chemotherapy before surgery to shrink the tumor and perhaps avoid a mastectomy; this is called neoadjuvant chemotherapy. Neoadjuvant therapy also allows for an early evaluation of the effectiveness of systemic therapy. In addition, neoadjuvant therapy may provide the opportunity to obtain tumor specimens and blood samples prior to and during the preoperative treatment. This has enabled researchers to identify tumor- or patient-specific biomarkers in order to plan appropriate targeted therapies (ACS, 2021j).
Statistically, chemotherapy treatment can reduce the relative risk of recurrence by about one fourth to one third. For example, a patient with a larger, more aggressive tumor and more lymph nodes involved might have a 75% chance of recurrence without chemotherapy. With chemotherapy, the statistical risk of recurrence might be reduced to around 50%. In contrast, a patient with a small tumor and negative lymph nodes might have a statistical risk of recurrence reduced from 12% to 8%. The higher the statistical risk of recurrence, the greater potential benefit from chemotherapy (NCCN, 2022a).
The medical oncologist generally quantifies a patient’s statistical risk of recurrence and the percentage of benefit the patient might expect from chemotherapy. This may be determined by pathology results and other information about the tumor, such as genomic information provided by the Oncotype DX test. This statistical analysis does not guarantee a particular outcome, and chemotherapy may have a greater or lesser effect on the risk of recurrence than predicted.
Common Treatment Regimens
Chemotherapy treatment is generally given in cycles of either every 21 or 28 days over the course of three months, six months, or one year, depending on the individual patient situation. The time between treatments allows the bone marrow to recover. At times, two or three different chemotherapy drugs are given in combination in order to increase effectiveness in eradicating cancerous cells (ACS, 2021j).
Oncologists have found that giving certain chemotherapy regimens closer together can lower recurrence rates and improve survival. Chemotherapy treatments are given as often as every two weeks with this regimen, called dose-dense chemotherapy. However, a dose-dense chemotherapy regimen can lead to more severe side effects and can be difficult to tolerate. Growth factors to help the white blood cell count recover may be given as well. Patients who are HER2-positive receive trastuzumab (Herceptin) on a weekly schedule, while receiving their chemotherapy every 21 days (ACS, 2021j).
In most situations, chemotherapy is most effective when combinations of one or more drugs are used. Many combinations are currently being used, and it is not clear that any single combination is the best. Clinical studies continue to compare current treatments with new agents and combinations.
| Name | Drugs |
|---|---|
| (ACS, 2021j; NCCN, 2022a) | |
| CMF | Cyclophosphamide (Cytoxan), methotrexate, and 5-fluorouracil |
| CAF (or FAC) | Cyclophosphamide (Cytoxan), doxorubicin (Adriamycin), and 5-fluorouracil |
| AC | Doxorubicin (Adriamycin) and cyclophosphamide (Cytoxan) |
| EC | Epirubicin (Ellence) and cyclophosphamide (Cytoxan) |
| TAC | Docetaxel (Taxotere), doxorubicin (Adriamycin), and cyclophosphamide (Cytoxan) |
| AC-T | Doxorubicin (Adriamycin) and cyclophosphamide (Cytoxan) followed by paclitaxel (Taxol) or docetaxel (Taxotere); trastuzumab (Herceptin) may be given with the paclitaxel or docetaxel for HER2/neu-positive tumors |
| CEF (or FEC) | Cyclophosphamide (Cytoxan), epirubicin (Ellence), and 5-fluorouracil; may be followed by docetaxel (Taxotere) |
| TC | Docetaxel (Taxotere) and cyclophosphamide (Cytoxan) |
| For HER2/neu-positive tumors | |
| TCH | Docetaxel (Taxotere), carboplatin, and trastuzumab (Herceptin) |
| AC-TH | Doxorubicin (Adriamycin), cyclophosphamide (Cytoxan), paclitaxel (Taxol), and trastuzumab (Herceptin) |
| AC-THP | Doxorubicin (Adriamycin), cyclophosphamide (Cytoxan), paclitaxel (Taxol), trastuzumab (Herceptin), and pertuzumab (Perjeta) |
| TCHP | Docetaxel (Taxotere), carboplatin , trastuzumab (Herceptin), and pertuzumab (Perjeta) TH Paclitaxel (Taxol) and trastuzumab (Herceptin) |
Different chemotherapy regimens are associated with particular risks and side effects, so it is important that each patient be informed and educated about the potential side effects of the regimen the oncologist recommends in order to make an informed decision about treatment. An instructional session that includes the significant other and/or caregiver by a knowledgeable, experienced oncology nurse or practitioner is crucial before chemotherapy commences. Other patients who have been through chemotherapy can be helpful resources as well, together with local support groups or online blogs, to help patients anticipate and cope with potential side effects.
Side Effects of Chemotherapy
Most chemotherapy drugs used to treat breast cancer have toxic side effects. Nausea and vomiting, hair loss, and fatigue are the most common. Increased risk of infection and anemia due to bone marrow suppression are other commonly seen toxicities and can actually become dose-limiting. Chemotherapy-induced menopausal symptoms, neuropathy, and cognitive changes are also frequent complaints.
NAUSEA AND VOMITING
Despite advances in antiemetic therapies, chemotherapy-induced nausea and vomiting (CINV) remains one of the most feared and expected side effects of chemotherapy. Preventive use of antiemetic therapy is important because CINV may lead to reduced quality of life, increased use of healthcare resources, and challenges to treatment adherence.
Healthcare professionals can be proactive in teaching coping skills for CINV. It can be helpful for patients to eat small, frequent meals and avoid foods that are fried, high in fat, strong tasting, strong smelling, gas forming, spicy, or acidic.
It is vital that caregivers are aware of the risk factors for severe nausea (female gender, young age, and vomiting during previous chemotherapy treatment) and that the patient knows to contact the healthcare provider promptly if CINV is not well-controlled. Studies show CINV is most successfully treated with a preventive, proactive approach.
HAIR LOSS
Generally speaking, if hair loss occurs, it will begin about 10 to 20 days after chemotherapy treatment begins. It can affect not only scalp hair but also body and facial hair, although eyebrows and eyelashes can take much longer to fall out. It is important to explain that the scalp needs protection with either a hat or sunscreen when exposed to the sun and in order to minimize loss of body heat when it is cold.
Usually, hair regrowth begins about three to six weeks after chemotherapy is completed. It is not uncommon for hair to grow back a different color or texture (known as “chemo-curl”), but typically, after about a year, it returns to its previous state. For older patients, however, if their post-chemo hair growth is white or grey, it may stay that color indefinitely.
FATIGUE
Fatigue is the most commonly reported side effect of chemotherapy. It is also the most debilitating side effect, affecting all other areas of a patient’s life. This distressing symptom may or may not be associated with anemia. There is much research concentrated on the exact physiologic cause of cancer-related fatigue and ways to combat it.
It is important for healthcare providers to assess fatigue levels using a fatigue scale (much like a pain scale) in order to evaluate the effectiveness of interventions and to be alerted to the potential for more serious problems (i.e., disease recurrence or progression) if the fatigue level is high.
Strategies to cope with cancer-related fatigue include:
- Prioritizing tasks and activities in order of importance
- Delegating errands and household chores to family and friends
- Taking short rest periods (20–30 minutes or less) during the day when needed
- Planning activities that require higher energy during peak energy times
- Incorporating moderate exercise (e.g., walking)
- Avoiding caffeine, as it can interfere with sleep
- Developing a bedtime routine to aid in sleep
- Taking in adequate fluids, as dehydration can contribute to fatigue
- Eating a balanced diet; limiting high-fat and high-sugar foods
(Gebruers, 2019; MSKCC, 2021)
Patients may also be encouraged to seek ways to decrease stress, which can contribute to fatigue, through relaxation techniques, quiet music, guided imagery, massage, meditation, etc.
INFECTION
Chemotherapy attacks rapidly dividing cancer cells. Unfortunately, it affects normal rapidly dividing cells as well.
White blood cells, a vital part of the immune system, are some of the most frequently dividing cells in the body, so they can be profoundly impacted by chemotherapy. Low white blood cell count (neutropenia, or low neutrophils) can result in decreased resistance to infection in people who are receiving chemotherapy.
For this reason, patients on chemotherapy treatments must be diligent in avoiding infection. The number-one preventive measure they and those in their households can take is frequent and thorough handwashing. A good reminder to give patients is to be sure hand hygiene is performed before eating, food preparation, and contact with eyes, nose, or mouth, and after using the toilet, contacting pets, and gardening.
Patients should also avoid crowds and people (especially children) with active colds or infections. Avoiding pet waste, such as changing cat litter boxes, is also recommended. Other precautions include prompt attention to cuts/injuries and to any signs of infection, wearing gloves while gardening, washing fruits and vegetables before consumption, and avoiding raw or undercooked animal products or seafood.
General signs and symptoms to watch for related to neutropenia include fever, chills, sweating, sore throat or sores in the mouth, abdominal pain, cough, and shortness of breath.
LIBIDO, INFERTILITY, EARLY MENOPAUSE
Chemotherapy can affect sexuality, intimacy, and fertility. It can cause vaginal dryness, pain, and discomfort during sexual activity. Premenopausal patients may experience infertility and early menopause induced by chemotherapy. The younger the patient, the more likely their menstrual periods will return when chemotherapy is finished. The closer they are to the age of natural menopause, the more likely chemotherapy will bring about menopause, with hot flashes, vaginal dryness, mood swings, and sleep disturbances. There may also be increased risk of osteoporosis.
Many of these factors, along with body image changes due to surgery and radiation, may impact a patient’s sexuality and intimacy. It is important to recognize and initiate a discussion about fertility and sexual changes as part of pretreatment education to address issues patients may face or are already experiencing. By normalizing the subject of intimacy and approaching it as a quality of life issue, healthcare providers may find patients become more comfortable in discussing their concerns. Patients with breast cancer should be encouraged to visit with a specialist in treating menopausal symptoms and sexual dysfunction that occurs as a result of the cancer or its treatments.
COGNITIVE EFFECTS
Many patients who have received chemotherapy treatment notice cognitive changes, or “chemo brain”—the forgetfulness, loss of concentration, and decrease in mental functioning that often accompany chemotherapy. Consequences of cancer treatment—such as low blood counts, fatigue, infection, menopause, poor nutrition, and sleep issues—may also trigger cognitive symptoms. The medical community recognizes these symptoms as real. Cognitive changes that begin during cancer treatment may last months and even years after treatment is complete.
CHEMOTHERAPY-INDUCED PERIPHERAL NEUROPATHY (CIPN)
Chemotherapy drugs used to treat breast cancer, including taxanes and platinum agents, can cause damage to the nerves, leading to peripheral neuropathy. The most common symptoms associated with CIPN are sensory neuropathies, including paresthesias (burning, tingling, and numbness) and pain starting in the fingers and toes, which can spread proximally. CIPN can begin weeks to months after initial treatment and reach a peak at or after the end of treatment. In some cases, the pain and paresthesias completely resolve after treatment is stopped. However, in most cases, CIPN is only partially reversible and can be permanent. CIPN may be prevented with the use of frozen gloves/socks worn during drug infusion with weekly paclitaxel.
TARGETED THERAPIES
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific cancer cells without harming normal cells. Monoclonal antibodies, tyrosine kinase inhibitors, cyclin-dependent kinase inhibitors, mammalian target of rapamycin (mTOR) inhibitors, and PARP inhibitors are types of targeted therapies used in the treatment of breast cancer (ACS, 2022c).
- Lapatinib (Tykerb) is a tyrosine kinase inhibitor that blocks the HER2 protein as well as other proteins inside tumor cells. It may be combined with other drugs to treat patients with HER2-positive breast cancer that has progressed after initial treatment with trastuzumab. When treatment with trastuzumab fails for patients with HER2-positive metastatic disease, lapatinib may improve progression-free survival. Lapatinib works by inhibiting intracellular cell signaling.
- Pertuzumab (Perjeta), like trastuzumab, is a monoclonal antibody that attaches to the HER2 protein. Pertuzumab targets a different part of the HER2 protein and can be used in combination with docetaxel and trastuzumab for first-line treatment in advanced-stage breast cancer patients.
- Ado-trastuzumab emtansine (Kadcyla) is a monoclonal antibody linked to a chemotherapy drug. This combination is called an antibody-drug conjugate. This drug is used to treat recurrent HER2-positive breast cancer.
- Naratinib (Nerlynx) is a tyrosine kinase inhibitor that blocks the HER2 protein as well as other proteins inside tumor cells. It is used to treat patients with early-stage HER2-positive breast cancer after initial treatment with trastuzumab.
- Palbociclib (Ibrance) is a cyclin-dependent kinase inhibitor used with the drug letrozole to treat recurrent breast cancer that is ER positive and HER2 negative. It is used in postmenopausal women whose cancer has not been treated with hormone therapy.
- Ribociclib (Kisqali) is a cyclin-dependent kinase inhibitor used with letrozole to treat recurrent or metastatic breast cancer that is hormone receptor positive and HER2 negative.
- Abemaciclib (Verzenio) is a cyclin-dependent kinase inhibitor used to treat hormone receptor–positive and HER2-negative breast cancer that is advanced or metastatic. It may be used alone or with other drugs.
- Everolimus (Affinitor) is a targeted therapy (for advanced HER2-positive or -negative cancers) that blocks mTOR, a protein in cancer cells that promotes growth. By blocking this protein, everolimus can stop cancer tumors from developing blood vessels and limit growth. Everolimus is usually given along with exemestance (Aromasin) in women who have disease progression while on either letrozole or anastrazole.
- Olaparib (Lynparza) is a PARP inhibitor used to treat patients with BRCA1 or BRCA2 mutations with HER2-negative metastatic breast cancer. PARP inhibitor therapy is also being studied for the treatment of patients with triple-negative breast cancer.
- Talazoparib (Talzenna) is a PARP inhibitor used to treat patients with BRCA1 or BRCA2 mutations with HER2-negative advanced-stage or metastatic breast cancer.
(ACS, 2022c)
BIOLOGIC THERAPY/HER-2 DIRECTED THERAPY
Rather than destroying cancer cells (and other cells), biologic therapy interrupts the tumor process. In 1998, research into biologic therapies showed promising results, and the FDA approved the drug trastuzumab (Herceptin) for metastatic breast cancer.
Fifteen to twenty percent of newly diagnosed breast cancers have amplification or overexpression of the HER2 oncogene (ACS, 2022c). Trastuzumab was a major breakthrough in the treatment of this usually aggressive tumor type, improving progression-free, disease-free, and overall survival.
Trastuzumab is a targeted approach to treatment that is classified as a monoclonal antibody. Originally FDA-approved for use in metastatic breast cancer, trastuzumab is now also approved and used as standard treatment in the adjuvant setting in combination with chemotherapy. Patients with HER2-positive breast cancer with nodal involvement and patients with HER2-positive tumors >2 cm without nodal involvement are appropriate candidates for first-line adjuvant treatment with trastuzumab. Patients with metastatic disease that is HER2-positive can also benefit from trastuzumab, sometimes as monotherapy, with very good results (NCCN, 2022a).
There are several types of epidermal growth factor receptors, but HER2 overexpression is most highly associated with breast cancer growth. Trastuzumab interrupts this cancer cell division by deactivating the protein on the surface of the cell that fuels its growth, in essence acting as a “false key” in the lock that fits the receptor but does not turn. The attached monoclonal antibody then also signals for cell destruction by the patient’s own immune system.
Side Effects and Contraindications
Because trastuzumab works differently than cytotoxic chemotherapy, it is not associated with the same side effects. Instead, the most common side effect appears to be infusion reactions—including shaking, chills, fever, headache, abdominal pain, and dyspnea, especially with the first dose—which can appear during infusion and up to 24 hours after infusion. Other possible but less common infusion reactions are vomiting, dizziness, rhinitis, hypotension, and rash.
Additional considerations are asthenia (loss of strength), left ventricular (LV) cardiac dysfunction, diarrhea, and increased incidence of leukopenia, anemia, neutropenia, and infection when used in combination with chemotherapy. Rarely, severe hypersensitivity reactions occur, in which case trastuzumab should be discontinued indefinitely. Also, pulmonary toxicities such as interstitial pneumonia and acute respiratory distress syndrome (ARDS) are uncommon but documented in patients receiving trastuzumab.
Because of the cardiac toxicity potential, patients who are to receive trastuzumab therapy are required to have either a multigated acquisition (MUGA) scan or a cardiac echocardiogram to determine baseline LV ejection fraction prior to start of therapy and at regular intervals throughout treatment. This monitoring is especially important for patients who also receive anthracyclines and/or chest irradiation. Patients must be educated to report urgently upon noticing any signs and symptoms of heart failure (ACS, 2022c).
Oncologists have specific guidelines for when to hold trastuzumab and when and how to restart therapy as testing shows improvement of LV function, although not standardized. Patients who have existing heart failure prior to treatment should not be started on trastuzumab, and those who show clinical signs of heart failure while on therapy should have therapy discontinued.
IMMUNOTHERAPY
Immunotherapy is a type of treatment that uses the patient’s own immune system to target the cancer. These substances are made both by the body or in a laboratory and used to direct the body’s defense system against the cancer. This type of treatment is also called biologic therapy.
Pembrolizumab (Keytruda) and Atezolizumab (Tecentriq) are PD-1 inhibitors used to treat metastatic breast cancer. PD-1 is a protein on the surface of T-cells that helps to keep the body’s immune system in balance. When PD-1 attaches to a protein on the surface of a cancer cell called PDL-1, it triggers the T-cells to attack the cancer cell (ACS, 2021k; NCCN, 2022a).
While generally well tolerated, immunotherapy can have significant adverse reactions that require prompt evaluation and treatment. Immune-related adverse events (IrAEs) occur when the over-activated immune system targets normal tissue and organs of the body. These events can occur anywhere in the body, but more common areas are the lungs (pneumonitis), skin (dermatitis), and thyroid (thyroiditis). Generally, the treatment for IrAEs is high-dose steroids with long, closely monitored tapers. Depending on the significance of the IrAE, therapy may need to be held or permanently discontinued (ACS, 2021k).
Integrative Care
Integrative therapies generally refers to strategies or treatments used in conjunction with conventional medicine as a complement to prescribed cancer treatment. The goal of these therapies is not to cure cancer but to work in concert with traditional cancer treatment to relieve symptoms and improve quality of life.
It is estimated that up to 80% of patients with cancer and long-term survivors of cancer use integrative therapies during and after cancer treatment (ASCO, 2022b). Many people with cancer choose one or more integrative therapies to reduce the side effects of chemotherapy and radiation, relieve pain, boost their immune system, improve quality of life, reduce stress, and promote healing. Integrative treatments can also help patients in coping with their cancer, as it can increase their sense of empowerment and wellness.
Integrative therapies may include nutritional supplements, dietary changes, herbal supplements, essential oils, exercise, yoga, tai chi, guided imagery, mindfulness meditation, massage, or acupuncture used in addition to conventional medicine. Nutritional supplements are the most frequently chosen therapy.
It is essential for healthcare professionals to obtain a complete list of all supplements a patient is utilizing to avoid possible interactions with or detrimental action against conventional cancer treatments. Assessment and monitoring throughout the illness trajectory is very important in protecting patient safety.
Unlike conventional medicine, which treats a specific problem by standard methods—such as surgery, radiation, or chemotherapy—integrative therapy views the patient as a whole entity and the body as more than the sum of its parts. More recently, this holistic approach has been referred to as mind-body medicine or integrative medicine.
Alternative therapies are unconventional treatments used in place of conventional, mainstream medicine. By definition, alternative therapies have not been scientifically proven, often have little or no scientific basis, and in some cases have even been disproved. Alternative therapies are too numerous and too controversial to address fully in this course. However, some common examples of alternative therapies for the treatment of cancer that patients may hear about include high-dose vitamin C, laetrile, and other herbal remedies.
Patients should be warned about the potential harm as well as the possible negative financial impact of using alternative therapy in place of evidence-based therapies exclusively for the treatment of cancer. The use of alternative therapies in place of conventional medicine may decrease the chance of remission or cancer cure. It is important to encourage a discussion of any and all treatment decisions in a nonjudgmental manner so as to keep the lines of communication open.
LIFESTYLE MANAGEMENT
Lifestyle management is a subspecialty that uses therapeutic lifestyle interventions as a primary modality to treat chronic conditions (ACLM, 2022). Pillars of this medical practice are informative to the whole-person care of those with breast cancer. These include physical activity, sleep hygiene, stress management, a nutritious diet, avoiding risky substances, and fostering positive social connections (ACLM, 2022).
Physical Activity
Physical activity is essential for recovery and maintaining good health. Regular physical activity after a cancer diagnosis can have a positive effect on quality of life, including physical (balance and flexibility), functional (reducing fatigue, improving heart and bone health), psychological, and emotional well-being (boosting energy and mood) (ACLM, 2022). It is recommended that cancer survivors engage in at least 150 minutes of moderate to vigorous physical activity each week. Activity should be spread out in shorter sessions each day, for example, 30 minutes most days of the week.
Patients on certain treatment regimens, such as those that may cause osteoporosis, are encouraged to incorporate regular weight-bearing exercise for bone health. Patients who have specific concerns or chronic conditions may benefit from a consultation with a physical therapist who can tailor a therapeutic fitness program designed for their unique needs during the treatment, recovery, and survivorship period.
The following are recommendations for discussing physical activity with patients with breast cancer:
- Encourage an initial discussion with their healthcare provider; focus on any long-term medical conditions.
- Plan a strategy; encourage patients to start slowly with 10-, 20-, and 30-minute sessions of some form of moderate activity each day. Encourage strength training as well as aerobic exercise.
- Choose activities patients enjoy; it is easier to stick with a plan when doing something enjoyable.
- Help patients explore new ways to exercise, including dancing, walking, climbing stairs, swimming, etc.
- Get the patient a pedometer (or step-counting app), since tracking progress can be a great way to see positive feedback.
- Encourage physical activity as a daily habit.
(NCCN, 2022b)
APPS FOR MAINTAINING A HEALTHY LIFESTYLE
There is emerging evidence that people with cancer can benefit in many ways from the use of mobile applications (apps) that focus on maintaining and improving the habits of a healthy lifestyle. Apps are available for smartphones or other devices to support self-management of pain, fatigue, psychological distress, and insomnia. As more evidence is reported on ways to leverage apps and other innovations in health and wellness technology, healthcare providers can incorporate these tools into the care of people with breast cancer (Silva, 2019).
Sleep Hygiene
Nearly half of patients with cancer report having problems with sleep. The most common issues are insomnia and abnormal sleep-wake cycles. Causes of sleep issues for people with breast cancer include:
- Physical changes from cancer surgeries or radiation (i.e., lymphedema)
- Side effects from medications used to treat or manage the symptoms of cancer (i.e., hormone therapy, corticosteroids, narcotics)
- Hospitalizations
- Stress
Managing issues with sleep can be difficult. However, some promising strategies include maintaining good sleep habits by ensuring a comfortable place to sleep, maintaining regular bowel/bladder habits, performing regular physical activity during the day, eating a well-balanced diet, and strategically timing medication administration (i.e., taking steroids in the morning).
Poor sleeping habits can contribute to other physical and mental issues. It is important for healthcare providers to routinely assess a patient’s sleep in order to effectively promote healthy sleep habits (NCI, 2022a).
Stress Management
Managing stress can be difficult for patients with breast cancer. Meditation and relaxation techniques can be successful ways to mitigate stress. Meditation is a simple form of relaxation that can be performed anywhere. Meditation and focused breathing can assist breast cancer patients during medical encounters such as procedures or chemotherapy administration. Meditation focuses on deep breathing with eyes closed for at least 5 to 10 minutes. Many patients find that adding soothing music or sounds can also help with relaxation.
Guided imagery is a form of meditation that includes forming a pleasant mental image to focus on while breathing deeply. Tai chi, described as a form of “moving meditation,” may also be appropriate as both a form of meditation and as gentle exercise (ASCO, 2022b).
Referrals to social work or other mental health services can be helpful for patients who have difficulty managing stress. Healthcare providers should routinely assess stress and explore factors contributing to stress in order to effectively direct patients to appropriate resources.
Nutrition
Nutrition is an incredibly important part of caring for people with breast cancer, particularly for those who are being treated with systemic therapies for extended periods of time and those recovering from surgical procedures or radiation.
Most healthcare practitioners agree that eating a healthful diet makes sense for anyone, and especially for people with breast cancer. Eating healthy can speed recovery, strengthen the immune system, restore energy, and reduce risk of cancer recurrence.
Eating a low-fat diet such as the Mediterranean diet may provide health benefits for cancer patients. The basic structure of the Mediterranean diet includes:
- Increased intake of fresh fruits and vegetables (7–10 servings per day)
- Use of whole grains (whole grain breads, cereals, and pasta)
- Use of olive oil instead of butter or margarine
- Adding herbs and spices instead of salt to enhance flavors
- Eating fresh fish and poultry instead of red meat
- Eating low-fat dairy products (e.g., Greek yogurt)
At times, nutritional drinks (e.g., Boost, Ensure) or enteral nutrition by way of a gastrostomy tube may be used to provide nutrients during acute cancer treatment when eating is difficult due to appetite changes, mucositis, and/or changes in taste. A referral to a registered dietitian can assist patients who have nutritional concerns during and after the treatment period.
VITAMINS AND MINERALS
Food is the best source of vitamins and minerals, but sometimes food fails to provide enough of certain nutrients, especially during recovery from cancer and its treatments.
More than half of all patients with cancer take one or more supplements, with or without their doctor’s approval. Common supplements used by patients include calcium and vitamin D for bone health, vitamins C and E for antioxidant effects, St. John’s wort for depression, garlic extract for blood pressure, and echinacea to enhance the immune system. Taking these supplements during treatment may interfere with or decrease the effectiveness of cancer-directed therapies (i.e., systemic therapy, radiation) (ASCO, 2022b).
- Patients should be cautioned not to take megadoses of vitamins and minerals because some vitamins can be toxic in large doses.
- Patients should be advised to discuss taking antioxidants such as vitamins C and E with their oncologist and integrative health practitioner. Patients may believe that taking antioxidants will enhance and protect their body’s normal cells, but use of antioxidants may also have a protective effect on tumor cells, thus making chemotherapy and radiation less effective. Radiation therapy and some types of chemotherapy work by generating free radicals to damage the DNA of tumor cells; taking antioxidants may block the therapeutic effect needed to kill tumor cells (ASCO, 2022b).
Supplement use is controversial because of limited research. However, the Office of Dietary Supplements at the National Institutes of Health was established in 1995 to create scientific databases on vitamins, minerals, and herbs (see “Resources” at end of course).
AVOIDING RISKY SUBSTANCES
It is important for people with breast cancer to main a healthy lifestyle by avoiding substances that are toxic or harmful. These include, but are not limited to, alcohol, smoking, illicit drugs, processed foods and preservatives, and other carcinogens/chemicals in food.
Fostering Positive Social Connections
Patients with breast cancer are often faced with radical changes to their lives as a result of the diagnosis. Few aspects of care are as important as maintaining positive relationships between the patient and their support system. A cancer diagnosis can place tremendous stress on these relationships. It is vital for the patient’s healthcare provider—and advocate—to connect patients and their loved ones to resources that maintain and foster positive social connections.
It is important for patients to pick the right time and place to break the news to their loved ones: time enough for asking and answering questions and a place where it is okay to cry, hug, and talk openly. Loved ones will be experiencing some of the same feelings as the patient—shock, fear, anger, and denial, plus empathy for the situation and sorrow at the possible loss this disease might cause. The patient is the only one who can decide whom to tell and how much to tell them. Some patients may not want to “go public” about their breast cancer but instead confine the news to immediate family and friends. Some patients cope by sharing their story openly with extended family and friends through social media such as Facebook or CaringBridge. The choice is very personal for each patient.
Family and friends may not know how to respond even though they may want to offer support. What they want most of all is for the patient to be okay again. Patients who explain their situation as they learn more about it can help loved ones deal with the news and show them how they might help. Patients may keep a list of those who offer, “Let me know if there’s anything I can do.” These people can be called on for help as needed: for a ride to medical appointments, to run errands, to prepare food, to help set up online tools for practical support issues, to care for children or pets, or just to drop by for a visit. Family and friends are often delighted to be of help.
Many patients fear that breast cancer will affect their relationships with others, particularly their sexual partners. This is particularly true for women who choose mastectomy; even some women who choose lumpectomy are surprised at the impact of the scar.
Concerns about relationships and sexuality can be particularly important to young women with breast cancer. Many young women are single and seeking to establish relationships. Almost all young women are working and just beginning to build a career. Some have no health insurance. Some are just starting families, and others have very young children. Young women also are likely to be diagnosed at a later stage and to have more aggressive tumors. Chemotherapy treatment may impair fertility and/or the ability to breastfeed if they do have children.
Many patients with breast cancer find comfort in talking with survivors and joining a professionally facilitated support group of people who are currently in treatment. Healthcare providers can provide resources to local support groups to patients when available.
OCCUPATIONAL THERAPY INTERVENTIONS
Occupational therapy (OT) practitioners are involved in all stages of cancer rehabilitation, including for patients with breast cancer. Research has confirmed the potential benefit of OT interventions in several broad areas.
Physical activity interventions:
- Exercise is safe and beneficial at all stages, including end of life, and regardless of age.
- Exercise, particularly aerobic exercise, reduces cancer-related fatigue.
- Exercise improves health-related quality of life (HRQOL).
- Diet and exercise interventions reduce the rate of self-reported functional decline.
- Exercise improves sleep quality for those undergoing cancer treatment.
Symptom management interventions:
- Nonpharmacologic interventions such as problem-solving, energy conservation, and education reduce the symptom of breathlessness.
- Sleep therapy modifications, education, and problem-solving for pain management and cognitive behavioral therapy are beneficial in managing cancer-related fatigue.
Psychosocial interventions:
- Cognitive-behavioral and educational interventions (e.g. problem-solving, knowledge of illness and side effects) reduce both anxiety and depression post treatment.
- Short-term life review increases spiritual well-being for people with terminal cancer.
- Stress management groups increases psychosocial adjustment among breast cancer survivors.
- Problem-solving therapy using home-based care training by phone helps women with breast cancer reduce stress.
- Self-management training in both group and individual environments improves quality of life.
- Expressive writing about one’s breast cancer experience improves quality of life outcomes, particularly for early-stage breast cancer survivors.
Rehabilitation programs that use a team approach including OT, PT, and other allied health professions improve function and participation regardless of stage of cancer or age of survivor.
(Hunter et al., 2017)
SURVIVORSHIP AND FOLLOW-UP CARE
Cancer casts a long shadow. Anyone diagnosed with cancer lives with the possibility of recurrence. Although many people survive breast cancer and live out a normal lifespan, others do not. That is why each new pain or other symptom may bring forth the fear of recurrence or metastasis until the symptom disappears or is found to be something other than cancer. Learning to live with uncertainty is part of recovery from cancer, and it is different for each individual. Healthcare professionals can help reduce the fear and anxiety associated with cancer survivorship by providing practical information to patients.
Patients should be encouraged to focus on wellness—taking good care of body, mind, and spirit—by eating a healthy diet, getting enough sleep and exercise, paying attention to symptoms, and getting regular checkups. Wellness also includes grieving one’s losses, whether the loss of a breast, loss of a relationship, or loss of the sense of control. It means seeking support when one needs it. Many patients continue with a support group after treatment has ended. Others seek individual counseling and psychological support. Many patients find further healing by helping others who are just starting on their cancer journey.
Survivorship Care Plan
The Commission on Cancer strongly encourages cancer centers to provide a survivorship care plan to all cancer patients. The American Cancer Society and American Society of Clinical Oncology both have published breast cancer survivorship care guidelines.
Breast cancer survivors may face significant short- and long-term effects of cancer and its treatment. To assist each survivor, an individualized care plan should be provided that includes a summary of all treatment, as well as a follow-up care plan. This plan is created in partnership with the cancer survivor to identify and prioritize individual goals. The survivorship care plan should also include information about individual risks, recommended tests and procedures, supportive care, and wellness strategies (ACS, 2022d). (See also “Resources” at the end of this course.)
Symptoms That Require Attention
If breast cancer recurs, it usually happens within the first five years after diagnosis and is most often suspected or discovered by patients themselves. ASCO (2021) recommends that breast cancer patients see their primary care provider immediately if any of the following signs and symptoms occur and/or persist:
- Chronic bone pain or tenderness (persistent)
- Bone fractures
- Skin rashes, redness, or swelling in the breast or arm (persistent)
- New lumps in the breasts, under the arm, or in the chest wall
- Changes in the shape or size of the breasts
- Chest pain and any shortness of breath (persistent)
- Pain that is constant, worsening, and not relieved by over-the-counter (OTC) medication
- Changes in weight, especially weight loss when not intentional
- Headaches that are not relieved by OTC medication
- Chronic cough or problems breathing
- Abdominal pain
- Jaundice (yellowing of skin and eyes)
- Changes in vision
- Extreme fatigue
- Poor appetite
- Fevers, night sweats
These symptoms may or may not be a sign of recurrence, but they do call for prompt evaluation.
Routine Follow-Up Care
Two major entities—ASCO (American Society of Clinical Oncology) and NCCN (National Comprehensive Cancer Network)—have issued guidelines for surveillance of breast cancer patients after curative-intent treatment.
ASCO guidelines (2021) include:
- History and physical exam every 3–6 months for 3 years, then every 6–12 months for 2 years, then annually thereafter
- Annual mammogram starting no sooner than 6 months after radiation therapy is completed
- Regular bone mineral-density testing for patients taking AIs
- Breast self-exam every month
- Continued treatment with endocrine therapy, as directed by oncologist
NCCN guidelines (2022c) mirror ASCO’s, except they recommend a history and physical exam every 4–6 months for 5 years, then annually thereafter.
Both guidelines recommend referral for genetic counseling for familial cancers. Both guidelines do not recommend any other routine laboratory tests or imaging unless abnormalities are detected with history and physical or mammogram because more intense surveillance has not been shown to improve overall survival.
These guidelines do not take into account a patient’s hormone receptor status. This is significant because hormone receptor–positive cancers are slower growing and may take longer to recur.
As the population of cancer survivors grows, additional research may lead to more accurate and specific guidelines.
Health and Wellness Recommendations
Patients recovering from breast cancer are encouraged to follow established wellness guidelines. These include maintaining a healthy weight, exercising, not smoking, and eating a balanced diet.
The following guidelines are encouraged:
- Eat a plant-based diet focused on fruits and vegetables, whole grains, and legumes; exclude high-calorie foods and beverages and consume less saturated fat.
- Include moderate physical activity for at least 150 minutes or vigorous activity for 75 minutes each week.
- Participate in strength-training exercises at least two days per week.
- Limit alcohol consumption to 0–1 drink per day, with no more than 7 per week.
- Quit smoking or using other types of tobacco.
- Follow recommendations for general cancer screening (see below).
(ASCO, 2021)
Other Cancer Screenings
Breast cancer patients must also stay current with screenings for other types of cancer, which may include colorectal, cervical (if cervix is present), endometrial (if uterus is present), and skin cancer, among others. Depending on age and family history, patients should be screened for colon cancer. If detected early, colorectal cancer can be completely cured by surgery to remove polyps. Women should have a Pap smear with HPV testing for detection of cervical cancer as often as directed by their healthcare provider. This is especially important in younger women. Cervical cancer is also highly curable when caught early, but it can be very deadly if not.
RECURRENT BREAST CANCER
Breast cancer that recurs may be local, regional, or metastatic. Treatment may be local/regional or systemic and can range from surgery alone to high-dose chemotherapy. The choice depends on several factors, including but not limited to:
- Location and size of the new tumor(s)
- Length of time since the initial cancer diagnosis
- Degree of lymph node involvement
- Whether distant organs are involved
Cancer that recurs within two years after the initial treatment tends to be more aggressive than cancer that recurs later.
Local Recurrence
Breast cancer most commonly recurs locally—in or near the site of the original tumor, for example in or around the scar. When recurrent cancer is confirmed, the physician orders blood tests and a bone scan to determine whether the cancer has spread beyond the breast. Any cancer that recurs locally is regarded as aggressive and resistant to treatment. When cancer recurs locally after lumpectomy, mastectomy is the preferred treatment.
Regional Recurrence
When breast cancer cells have spread to the adjacent lymph nodes (usually in the axilla) or to the chest wall, it is termed a regional recurrence. This may require surgical treatment and/or localized radiation therapy as well as systemic treatment.
Cancer in a different part of the breast or in the contralateral (opposite) breast may be a new cancer, which is called a second primary cancer. This cancer may be an entirely different cell type and may be treated successfully with surgery alone, depending on the stage and tumor type. The biopsy may or may not be able to determine whether the new tumor is recurrent disease or a second primary, but it will help determine the treatment.
Metastatic Disease (Distant Metastasis)
Once breast cancer has spread to distant organs (stage 4), cure is no longer possible. However, palliative care measures—including radiation, chemotherapy, endocrine therapies, targeted therapies, and bisphosphonates—can significantly improve survival length and quality of life. The most common sites of metastasis for breast cancer are the bone, brain, lungs, and liver.
Breast cancer that metastasizes to the bone can be treated with targeted radiation therapy, either via stereotactic external beam or with radiopharmaceuticals. Therapies such as pamidronate (Aredia), zoledronic acid (Zometa), and denosumab (Xgeva, Prolia) can help reduce the pain of bone metastases, strengthen bones, and decrease morbidity due to skeletal-related events (SREs). There may be the need for surgical intervention, in some cases for rod placement, to either treat or prevent fracture in large, weight-bearing bones that are affected by disease. Patients with cancer in the bone should be cautioned about the increased risk of fracture (Eisen, 2022).
Metastatic cancer that develops in the brain or around the spinal cord can also be treated to improve quality of life. Steroid medications can be given to decrease pain, swelling, and neurological symptoms. Whole brain radiation or localized brain radiation (Gamma Knife treatment) can be used to treat patients whose cancer has spread to the brain.
Palliative Care
Palliative care can be offered during this time. Palliative care specialists work together with the healthcare team, such as nurses, nutritionists, social workers, chaplains, pharmacists, and others, to focus on creating an individual plan to address any lasting treatment side effects, pain, emotional aspects, and other concerns of the cancer patient. The idea is to treat the whole person—including the physical, emotional, social, and spiritual.
Palliative care is often confused with hospice care, which is provided for people who have a terminal diagnosis. Palliative care can be provided at any time during a cancer diagnosis, not just at the end of life.
The inclusion of palliative care may include positive benefits such as:
- Ability to fully complete treatment
- Improved quality of life during treatment
- Increased ability to perform daily activities
- Living longer
- Improved ability to respond to emotions
- Increased connection to social support
- Fewer hospitalizations
WHEN CURE IS NO LONGER POSSIBLE
When efforts to slow cancer growth are no longer effective, emphasis shifts from cure or control of the cancer to providing comfort and symptom management with a goal of providing the best quality of life possible. For many patients, making the decision to stop cancer treatment that is no longer working can be a powerful step to be free of the side effects of treatment and take control of their lives.
Patients with recurrent or metastatic breast cancer require support and understanding more than ever, not only from family and friends but from healthcare professionals as well. They need to be able to talk openly about their cancer, feelings and concerns, care preferences, and decisions about ending treatment. Helping patients and their family members change their focus from seeking cure to seeking the best comfort and quality-of-life measures with end-of-life care is paramount. Because this can be very stressful for some people, they may require support from various resources, such as social work, certified counseling/psychotherapy, peer support groups, and chaplains.
Cancer reminds us to take care of unfinished business, not only in personal relationships but also in practical matters, sometimes referred to as “getting one’s affairs in order.” Although family and friends may be uncomfortable with these discussions, they can be reassuring to the patient.
WAYS TO MAINTAIN HOPE AND CONNECTION TO OTHERS
- Encourage quality time with family (plan a trip or outing that they have always wanted to take together)
- Focus on pain and symptom management
- Encourage expression of feelings (communicating their love for others, forgiveness, and/or gratitude)
- Create a living legacy to leave for family members (writing letters or recording family stories or videotaped messages)
- Encourage time with friends who are supportive
ELEMENTS OF PRACTICAL END-OF-LIFE PLANNING
- Advance medical directives
- Do-not-attempt-resuscitation (DNAR or DNR) or allow natural death (AND) orders
- Legal issues such as wills and estate planning
- Hospice care
- Organ donation
- Legacy building
- Funerals and memorials
Hospice Care
Hospice care is provided for people once they receive a terminal diagnosis. The hospice team usually includes doctors, nurses, pharmacists, social workers, therapists, chaplains, and others. The goal of hospice is to provide the best quality of life during the time remaining and to allow the patient and family to have a peaceful and natural death experience.
People may mistakenly think that hospice refers to a place. Although there are some residential hospice facilities, most hospice care takes place in the client’s home or the home of a loved one, with family members participating in care if they choose. However, hospice care also occurs in hospitals and nursing home settings.
Often, when patients have reached a place of acceptance about nearing the end of life, they can be very peaceful about it but still fearful of death itself being painful. At this stage in the patient’s care, it is important to ensure that the level of pain control is satisfactory for the patient. Hospice nurses especially are trained in this area and work closely with the patient and physician in utilizing medications and strategies available to attain the best pain control possible while minimizing unwanted side effects.
Nurses and other healthcare professionals can provide information and resources to help friends and family members understand why implementing hospice care does not mean that the patient is “giving up” and may actually be comforting to the patient. For example, some people think calling in hospice will shorten the patient’s survival. However, patients who receive hospice care many times live longer than those who do not have hospice care.
No matter where patients are in their breast cancer journey, all healthcare professionals can empower them to cope in the best manner possible through individualized education, skilled care, encouragement, and support.
CONCLUSION
Breast cancer is a common malignancy among women, representing 4 in 10 female cancer survivors in the United States. Long-term survival is common after breast cancer treatment, with a 5-year survival rate of 90% (ACS, 2022a).
Diagnosis and treatment for breast cancer may vary based on many factors, including type, stage, and other individual differences. Patients may be presented with various treatment options and need expert guidance to assist in decision making, weighing short- and long-term effects of each treatment choice. For most, treatment does not end with the initial surgery, radiation, and/or chemotherapy but may include long-term surgeries for reconstruction as well as endocrine therapy for a period of 5 to 10 years to prevent recurrence.
Survivorship for individuals with a history of breast cancer may include monitoring and surveillance of short- and long-term effects of treatment as well as screening for other secondary cancers. Patients who are actively involved in their care, with a focus on wellness goals—including nutrition, mind-body strategies, and exercise—may experience a better quality of life and have a decreased chance of cancer recurrence (ASCO, 2021).
As patients live longer with breast cancer and the associated long-term treatments, care has shifted to a chronic care model. People with a history of breast cancer will benefit from the initiation of standards and expectations to provide patients with an individualized survivor care plan to assist them in being as informed as possible about their future.
RESOURCES
Breast cancer survivorship (Cancer.net)
Breast cancer risk assessment tool
CancerCare (counseling, support, education, financial assistance)
ClinicalTrials.gov (National Institutes of Health)
National Cancer Institute (National Institutes of Health)
NCCN practice guidelines in oncology (National Comprehensive Cancer Network)
Office of Dietary Supplements (National Institutes of Health)
REFERENCES
NOTE: Complete URLs for references retrieved from online sources are provided in the PDF of this course.
American Cancer Society (ACS). (2022). Inflammatory breast cancer. https://www.cancer.org
American Cancer Society (ACS). (2022a). Key statistics for breast cancer. https://www.cancer.org
American Cancer Society (ACS). (2022b). Second cancers after breast cancer. https://www.cancer.org
American Cancer Society (ACS). (2022c). Targeted therapy for breast cancer. https://www.cancer.org
American Cancer Society (ACS). (2022d). Follow-up care after breast cancer treatment. https://www.cancer.org
American Cancer Society (ACS). (2021a). Breast cancer stages. https://www.cancer.org
American Cancer Society (ACS). (2021b). Hormone therapy for breast cancer. https://www.cancer.org
American Cancer Society (ACS). (2021c). Imaging tests to find out if breast cancer has spread. https://www.cancer.org
American Cancer Society (ACS). (2021d). Invasive breast cancer. https://www.cancer.org
American Cancer Society (ACS). (2021e). Lymph node surgery for breast cancer. https://www.cancer.org
American Cancer Society (ACS). (2021f). Paget disease of the breast. https://www.cancer.org
American Cancer Society (ACS). (2021g). Radiation for breast cancer. https://www.cancer.org
American Cancer Society (ACS). (2021h). What is lymphedema? https://www.cancer.org
American Cancer Society (ACS). (2021i). Lifestyle-related breast cancer risk factors. https://www.cancer.org
American Cancer Society (ACS). (2021j). Chemotherapy for breast cancer. https://www.cancer.org
American Cancer Society (ACS). (2021k). Immunotherapy for breast cancer. https://www.cancer.org
American College of Lifestyle Medicine (ACLM). (2022). What is lifestyle medicine? https://www.lifestylemedicine.org
American Occupational Therapy Association (AOTA). (2021). Occupational therapy’s role across the continuum of care for patients with breast cancer. https://www.aota.org
American Society of Clinical Oncology (ASCO). (2022a). Breast cancer—inflammatory: Statistics. https://www.cancer.net
American Society of Clinical Oncology (ASCO). (2022b). Integrative medicine. https://www.cancer.net
American Society of Clinical Oncology (ASCO). (2021). Breast cancer: Follow-up care and monitoring. https://www.cancer.net
Brown J, Scardo S, Method M, Schlauch D, Misch A, Picard S, Hamilton E, et al. (2022). A real-world retrospective study of the use of Ki-67 testing and treatment patterns in patients with HR+, HER2- early breast cancer in the United States. BMC Cancer, 22(502). https://doi.org/10.1186/s12885-022-09557-6
Center for Disease Control and Prevention (CDC) (2022). Triple-negative breast cancer. https://www.cdc.gov
Eisen A, Somerfield M, Accordino M, Blanchette P, Clemons M, Dhesy-Thind S, Dillmon M, et al. (2022). Use of adjuvant bisphosphonates and other bone-modifying agents in breast cancer: ASCO-OH (CCO) guideline update. Journal of Clinical Oncology, 40(7), 787–800. https://doi.org/10.1200/JCO.21.02647
Gebruers N, Camberlin M, Theunissen F, Tjalma W, Verbelen H, Soom T, & Breda, E. (2019). The effect of training interventions on physical performance, quality of life, and fatigue in patients receiving breast cancer treatment: A systematic review. Supportive Care in Cancer, 27(1), 109–22. https://doi.org/10.1007/S00520-018-4490-9
Giuliano AE, Edge SB, & Hortobagyi GN. (2018). Eighth edition of the AJCC cancer staging manual: Breast cancer. Annals of Surgical Oncology, 25(7), 1783–5.
Hunter EG, Gibson RW, Arbesman M, & D’Amico M. (2017). Centennial topics—Systematic review of occupational therapy and adult cancer rehabilitation: Part 1. Impact of physical activity and symptom management interventions. American Journal of Occupational Therapy, 71, 7102100030. https://doi.org/10.5014/ajot.2017.023564
Hunter EG, Gibson RW, Arbesman M, & D’Amico M. (2017). Centennial topics—Systematic review of occupational therapy and adult cancer rehabilitation: Part 2. Impact of multidisciplinary rehabilitation and psychosocial, sexuality, and return-to-work interventions. American Journal of Occupational Therapy, 71, 7102100040. https://doi.org/10.5014/ ajot.2017.02357
Koesterts J. (2021). Breast cancer recovery and lymphedema: How physical therapy can help. https://dickinson.rehabvisions.com
Manahan M. (2022). Breast cancer: Lymphedema after treatment. https://www.hopkinsmedicine.org
Memorial Sloan Kettering Cancer Center (MSKCC). (2022). Lymphedema treatment after breast cancer. https://www.mskcc.org
Memorial Sloan Kettering Cancer Center (MSKCC). (2021). Managing cancer-related fatigue with exercise. https://www.mskcc.org
Mutter RW, Choi JI, Jimenez RB, Kirova YM, Fagundes M, Haffty BG, Amos RA, et al. (2021). Proton therapy for breast cancer: A consensus statement from the particle therapy cooperative group breast cancer subcommittee. International Journal of Radiation Oncology*Biology*Physics, 111 (2), 337–59. https://doi.org/10.1016/j.ijrobp.2021.05.110
National Cancer Institute (NCI). (2022). Breast cancer treatment (Adult) (PDQ): Health professional version. https://www.cancer.gov
National Cancer Institute (NCI). (2022a). Sleep disorders: Health professional version. https://www.cancer.gov
National Cancer Institute (NCI). (2021). Radiation therapy and you: Support for people with cancer. https://www.cancer.gov
National Comprehensive Cancer Network (NCCN). (2022a). Breast cancer. https://www.nccn.org
National Comprehensive Cancer Network (NCCN). (2022b). Supportive care. https://www.nccn.org
National Comprehensive Cancer Network (NCCN). (2022c). Survivorship. https://www.nccn.org
Silva E, Lawler S, & Langbecker D. (2019). The effectiveness of mHealth for self-management in improving pain, psychological distress, fatigue, and sleep in cancer survivors: A systematic review. Journal of Cancer Survivorship, 13, 97–107. https://doi.org.10.1007/s11764-018-0730-8
Vinogradova Y, Coupland C. & Hippisley-Cox J. (2020). Use of hormone replacement therapy and risk of breast cancer: Nested case-control studies using the QResearch and CPRD databases. BMJ, 371, 1–16. https://doi.org/10.1136/bjm.m38873
Customer Rating
3.8 / 545 ratings