Child Abuse Mandated Reporter Training for New York State
Identifying and Reporting Child Abuse and Maltreatment
Online Continuing Education Course

Course Description
New York State Education Department (NYSED) Mandate: In 2025, Section 413 of the New York Social Services Law was amended to require the addition of guidance on identifying an abused or maltreated child when such child is an individual with an intellectual or developmental disability. This course has been updated to include the additional content. New York law requires every person who is required to take the mandated training related to child abuse, including those who have previously undergone this training, to complete this updated training by November 17, 2026.
Course Price: $30.00
Contact Hours: 2
Course updated on
September 1, 2025
"I read another vendors pdf class and selected NOT to take their class due to the lack of information flow and disconnect in test questions. Glad I moved on to Wild Iris to complete my NYS mandatory." - Linda Dobson, RN in New York
"Even though I have taken mandated reporting courses several times in the past, this course provided new information pertinent to my employment and profession." - Tanya, LPN in New York
"Everything was very clearly laid out and understandable. Coming from out of state, this definitely helped clarify the New York reporting laws." - Allyssa, teacher in New York
"This course came highly recommended to me. I am confident in my newly acquired skills and I am glad I took it." - Stephanie, RN in New York
Updated 2024 and updated 2025 with the mandated reporter training syllabus to include recent amendments to Social Services Law paragraph 413 requiring the addition of coursework on adverse childhood experiences and trauma, implicit bias, and recognition of child abuse virtually, and with the addition of guidance on identifying an abused or maltreated child when such child is an individual with an intellectual or developmental disability. This course fulfills the updated requirement for training in identifying and reporting child abuse, maltreatment, and neglect in New York. We are a NYSED-approved provider.
Child Abuse Mandated Reporter Training for New York State
Identification and Reporting Child Abuse and Maltreatment/Neglect
Copyright © 2025 Wild Iris Medical Education, Inc. All Rights Reserved.
LEARNING OUTCOME AND OBJECTIVES: Upon completion of this course, you will have gained the knowledge to identify and report child abuse, neglect, and maltreatment. Specific learning objectives to address potential knowledge gaps include:
- Understand the impacts of trauma and adverse childhood experiences (ACEs).
- Identify protective factors against trauma.
- Discuss implicit bias and its relationship to child welfare.
- Summarize New York definitions pertaining to child abuse and maltreatment.
- Recognize indicators of child maltreatment and abuse, including in a virtual setting.
- Describe New York State reporting requirements, including calling the Statewide Central Register (SCR) and filing the Form LDSS-2221A.
- Discuss the legal protections afforded mandated reporters and the consequences for failing to report.
TABLE OF CONTENTS
Content in this course is adapted from the 2025 New York State Mandated Reporter Training Syllabus.
INTRODUCTION
The abuse or maltreatment of children is against the law. The government has a responsibility to protect children when parents or other persons legally responsible for a child’s care fail to provide proper care and to intervene in cases of child abuse or maltreatment. Likewise, healthcare professionals have a responsibility to recognize and report suspected child abuse and maltreatment.
In New York, Child Protective Services (CPS) operates in each county and is required to investigate child abuse and maltreatment reports; to protect children (anyone under 18 years old) from further abuse or maltreatment; and to provide rehabilitative services to children, parents, and other family members involved.
The New York State Office of Children and Family Services (OCFS) maintains the Statewide Central Register (SCR) of Child Abuse and Maltreatment (which is a 24-hour hotline). The SCR receives calls alleging child abuse or maltreatment within New York State and relays information to the local CPS for investigation, monitors their prompt response, and identifies whether there are prior child abuse or maltreatment reports.
Certain persons are required by law (mandated) to report suspected child abuse or maltreatment to the SCR. Nonmandated reporters, including the public, may also contact the SCR. Examples of mandated reporters include, but are not limited to:
- Medical and hospital personnel
- School officials
- Social service workers
- Childcare workers
- Residential care workers and volunteers
- Law enforcement personnel
(NYS OCFS, n.d.-a)
Mandated reporters are legally obligated to call the SCR only in certain circumstances (see “What Situations Require That a Report Be Made?” later in this course).
In other instances, families in crisis may not meet the legal criteria required to call the SCR. When a mandated reporter finds a family in crisis and the children are not in imminent danger of harm, it is best to assess the situation to see if the family could benefit by being connected to community services in their area. Such resources include:
- HEARS Family Line, 888-55HEARS (544-3277) (Help, Empower, Advocate, Reassure and Support): Resources and referrals to services such as food, clothing, housing, childcare, parenting education, and more, available Monday through Friday, 8:30 am to 4:30 pm, with messages in 12 languages
- Child Welfare and Community Services: Online listing of resources and available services, at https://ocfs.ny.gov/programs/cwcs/aces.php
- NY Project Hope: Emotional support, including the Emotional Support Helpline (1-844-863-9314), online wellness groups, and online listing of supportive resources, at https://NYProjectHope.org
- New York State Office for the Prevention of Domestic Violence: Online listing of resources for those experiencing, or survivors of, domestic violence, at https://opdv.ny.gov/survivors-victims
- Prevent Child Abuse New York: Prevention and parent helpline (1-800-CHILDREN), confidential and multilingual, including referrals to caregivers to community-based services, available Monday through Friday, 9 am to 4 pm
- 2-1-1 (operated by the United Way): Health and human services information, referrals, assessments, and crisis support, multilingual and available 24 hours a day
(NYS OCFS, 2025)
(See “Resources” at the end of this course for a link to the “Summary Guide for Mandated Reporters.”)
UNDERSTANDING TRAUMA AND ADVERSE CHILDHOOD EXPERIENCES
Trauma may impact a child or family, and its effects may become apparent to the many professionals who are mandated reporters of child abuse and maltreatment. A reporter’s own past experiences with trauma may also impact their decision-making.
It is important to remember that trauma alone may not rise to the level of child abuse or maltreatment and that it is the impact on the child that should be assessed by the mandated reporter. Many effects of trauma and adverse childhood experiences can be addressed by supporting children and families and increasing protective factors against these effects (NYS OCFS, 2025).
Trauma
Trauma is an intense event that threatens a person’s life or safety in a way that is too much for the mind to handle and leaves the person powerless. Trauma can bring about physical reactions such as rapid heart rate, tense muscles, or shallow breathing. Common traumatic events could be going through or seeing:
- Family violence
- Sexual abuse
- Emotional abuse
- Violence in the community
For many parents, having a child removed from the home and dealing with the child welfare system are traumatic events. In that way, trauma impacts the work of a mandated reporter in addressing possible child maltreatment or abuse.
Adverse Childhood Experiences (ACEs)
Adverse childhood experiences (ACEs) are negative experiences that occur during childhood. Research has shown that ACEs can have lasting impacts on physical, emotional, and mental health throughout a person’s life. Research shows that ACEs are very common in all socioeconomic groups; 61%–67% of the U.S. population has experienced at least one ACE.
Children who have experienced numerous adverse experiences have higher rates of negative health outcomes, including depression, obesity, substance use, anxiety, heart disease, and early death. Other factors can intensify the effects of ACEs, including poverty, racism, generational trauma, and frequent unintended or indirect discrimination. Child maltreatment and abuse are adverse childhood experiences (NYS OCFS, n.d.-b).
Toxic stress occurs when a person experiences severe, prolonged adversity without adequate support. Toxic stress means that the stress response stays continuously activated in the body. Toxic stress impacts children developmentally and behaviorally.
(See “Resources” at the end of this course for more information on ACEs.)
Trauma-Informed Practice
Trauma-informed practice is a model for engaging with individuals and families that recognizes the impact and influence that trauma may have on them. Goals of a trauma-informed practice are to avoid the inadvertent retraumatization of individuals through one’s own interactions with them and to understand that trauma may have an impact on a person’s behavior.
Trauma-informed practice includes identifying one’s own past experiences or trauma and understanding how they may impact how one evaluates and makes decisions regarding an incident encountered in one’s professional capacity.
Six key elements of a trauma-informed approach include:
- Safety. The provider ensures safety for the patient, both physical and emotional, and maximizes the patient’s control. The provider aims to meet the basic needs of the patient, including necessary medications.
- Trustworthiness and transparency. The provider spells out the limits of confidentiality and ensures that the patient is heard and understood.
- Peer support. The provider encourages the patient to implement self-help by engaging in treatment with a team that includes others with lived experience.
- Collaboration and mutuality. The provider acknowledges the individual roles of the patient and staff and attempts to even out power discrepancies.
- Empowerment, voice, and choice. The provider supports the individual’s sense of agency and helps the survivor become empowered.
- Cultural, historical, and gender issues. The provider recognizes that there may be sources of trauma from cultural, racial, ethnicity, gender, and historical issues, including adverse childhood experiences (ACEs).
(HTC, n.d.)
Resilience and Protective Factors
The ability to bounce back from challenges and hardship is called resilience. This quality has been shown to reduce the negative impacts of ACEs in both parents and children. Certain protective factors can boost resilience in both parents and children. These include:
- Supportive and caring relationships and social connections
- Programs that understand a person’s background and culture
- A healthy lifestyle (e.g., regular exercise, mindfulness, sufficient sleep, a healthy and nutritious diet)
- Economic support/stability for families
- Quality childcare and education early in life
(NYS OCFS, n.d.-b)
Professionals can help reduce the effects of ACEs by supporting children and families to increase these protective factors.
UNDERSTANDING AND REDUCING IMPLICIT AND EXPLICIT BIAS
Bias and prejudice have existed since ancient times. Most of the documented occurrences of bias describe overt or conscious bias. It is only fairly recently that the concept of implicit bias has been described. In 1995, psychologists Mahzarin Banaji and Anthony Greenwald used the term implicit bias to describe “social behavior [that] often operates in an implicit or unconscious fashion. The identifying feature of implicit cognition is that past experiences influence judgment in a fashion not introspectively known by the actor” (UCC, 2022).
What Is Bias?
Biases are attitudes, behaviors, and actions that are prejudiced in favor of or against a person or group. Implicit bias, also known as unconscious bias, is a form of bias that is both automatic and unintentional. It may include stereotypes, judgments, and assumptions that someone unknowingly believes are true and that may be based on factors such as age, race, weight, gender, gender orientation, sexual orientation, religion, socioeconomic status, or more.
Although people with implicit biases are unaware of their prejudices, these biases may still affect their behaviors and decisions. Another important facet of implicit bias is that it is not only outside of the person’s awareness, but it may directly contradict what they verbalize as their beliefs and values (NIH, 2022; Maryville University, n.d.).
Becoming aware of one’s biases and their potential impacts allows a person to take a proactive role in reducing how biases may impact their decision-making.
DIFFERENTIATING BETWEEN EXPLICIT AND IMPLICIT BIAS
Explicit bias, also known as conscious bias, is overt and easily recognized. People who have explicit biases are very much aware of their feelings, attitudes, and behaviors, which are typically presented with intent. In its extreme, explicit bias is characterized by “overt negative behavior that can be expressed through physical and verbal harassment or through more subtle means such as exclusion.”
Implicit bias, however, is outside of a person’s awareness. Unlike explicit bias, it can automatically, progressively, and adversely affect behavior in a manner that is not immediately apparent and outside a person’s consciousness (NCCC, n.d.).
Impact of Implicit Bias in Child Welfare
Disparities exist throughout the child welfare system presently and historically. In New York State, OCFS Disproportionate Minority Representation (DMR) data shows that children and families of color are overrepresented in the child welfare system. Families of color have been more likely to have been involved in a report to the SCR. Children of color have been more likely to have been placed in foster care.
The income status of families is also a significant predictor of involvement with the child welfare system. While poverty does not equate to child abuse or maltreatment, families investigated by CPS have several poverty-related risk factors such as unemployment, single parenthood, food insecurity, housing stability, or lack of access to childcare. Families living below the poverty line are three times more likely to be substantiated for child maltreatment (NYS OCFS, 2025).
Strategies to Reduce Implicit Bias
A mandated reporter’s decision to call the SCR can change the course of the life of a child and family members and have long-lasting and devastating impacts on both families and communities. Therefore, it is important for professionals to be aware of the potential for implicit biases and to ensure that such biases do not impact their decision-making. Instead, decisions must be made based on the objective facts of a situation.
A proven strategy to reduce bias and increase awareness regarding one’s own beliefs is to ask oneself the question, would I make a different decision to call the SCR if the child or family in a situation of suspected of child maltreatment or abuse were of a different:
- Race?
- Ethnicity?
- Sex assigned at birth?
- Gender identity or expression?
- Sexual orientation?
- Religion?
- Immigration status?
- Primary spoken language?
- Culture?
- Age?
- Neighborhood where they reside?
- Presence of a disability?
- Occupation?
- Socio-economic status of the family?
If the answer is yes, bias may be impacting the decision to call the SCR.
Another strategy when assessing information received about a child and their family is to ask analytical and evaluative questions and use critical thinking. This includes:
- Identifying the specific concerns about the current situation
- Gathering adequate information about the current situation
- Analyzing that information to separate facts from assumptions
- Recognizing the possibility of bias in one’s personal opinions
- Developing multiple hypotheses that could explain the situation
- Determining whether calling the SCR is legally required
- If not, determining whether an alternative option is better, such as connecting the individual or family to appropriate services in their community
Often, it is possible to support a family without reporting a family to the CPS system. Mandated reporters must approach this responsibility with empathy, compassion, care, and curiosity (NYS OCFS, 2025).
HARVARD IMPLICIT ASSOCIATION TEST
One way to develop self-awareness is through the use of an educational tool. The Harvard Implicit Association Test (IAT) was created in 1998 for the purpose of measuring and detecting a person’s implicit bias. The test can be used to measure biases in relation to race, sexual orientation, gender, age, and various other categories. This test has been found to offer some insight into how groups of people with different traits, behaviors, and cultures are viewed by others.
The IAT takes about 10–15 minutes to complete and can be accessed on the Project Implicit website (see “Resources” at the end of this course). Participants are asked to sort and categorize a variety of images and words and respond to a questionnaire related to the topic. The strength of association between the various types of content is measured based on how quickly the user reacts to the associations (MAEPD System, n.d.). Results are classified as no bias, slight bias, moderate bias, or strong bias toward people of different races, sexual orientations, and other bias-related categories.
The IAT is not a perfect measurement of implicit bias. There are some criticisms, including the fact that people may take the test multiple times and provide different answers or that various issues could influence someone’s reaction time while taking the test. However, the test results are a good way to start introspection and the process of self-awareness (Practical Psychology, 2022).
DEFINING MALTREATMENT AND ABUSE
Different states and government entities may vary in their definitions of child abuse. The following definitions are specific to the state of New York and address various forms of abuse.
Person Legally Responsible (PLR)
The New York State Family Court Act, Section 1012(g), states:
“Person legally responsible” includes the child’s custodian, guardian, or any other person responsible for the child’s care at the relevant time. Custodian may include any person continually or at regular intervals found in the same household as the child when the conduct of such person causes or contributes to the abuse or neglect of the child.
Abuse
Child abuse may include serious physical harm or substantial risk of serious physical harm to the child. Acts of sexual abuse are also included in this definition. These acts are committed by the parents or caretakers of the child or allowed to occur by the parent or caretaker.
Child abuse in New York State is defined in Family Court Act, Section 1012(e) (emphasis added).
“Abused child” means a child less than 18 years of age whose parent or other person legally responsible for the child’s care:
- Inflicts or allows to be inflicted upon such child physical injury by other than accidental means which causes or creates a substantial risk of death, or serious or protracted disfigurement, or protracted impairment of physical or emotional health, or protracted loss or impairment of the function of any bodily organ; or
- Creates or allows to be created a substantial risk of physical injury to such child by other than accidental means which would be likely to cause death or serious or protracted disfigurement, or protracted impairment of physical or emotional health, or protracted loss or impairment of the function of any bodily organ; or
- Commits or allows to be committed a [sex] offense against such child … [see “Sexual Abuse” below]
Neglect
Child neglect in New York State is defined in the Family Court Act, Section 1012(f). Neglect can be physical, mental, or emotional. It includes the failure of a parent or person legally responsible (PLR) to provide a child with the minimum degree of care for normal growth and development. This includes:
- Adequate food
- Adequate clothing
- Adequate shelter
- Adequate medical care (basic dental care, mental health services, treatment for drug or alcohol misuse)
- Adequate education (ensuring the child is actively enrolled in school)
- Adequate supervision
- No excessive corporal punishment
The minimum degree of care regarding adequate food, clothing, shelter, and medical care must be considered in regard to whether the parent or PLR was financially able to do so or was offered other financial or reasonable means to do so.
Being actively enrolled in school does not mean a child has to be earning high grades, participating in activities, or have perfect attendance. The minimum degree of care is measured according to the conduct of the parent after considering any efforts previously made by the school or Child Protective Services.
There is no provision in New York State law or regulation that dictates how old a child must be to be left alone without adult supervision. Determining whether a child can be safely left alone must be made on a case-by-case basis as demonstrated by the child’s knowledge and skills necessary to properly respond to a potential emergency and to care for themselves. Just because an individual child may be left safely alone does not mean that child has the necessary skills to supervise other children without an adult present.
New York State law permits parents to use corporal (physical) punishment to discipline their children, but it cannot be excessive. Excessive corporal punishment includes when:
- The child lacks the capacity to understand the corrective quality of the discipline.
- A less severe method is available and likely to be effective.
- The punishment is inflicted due to the parent’s rage.
- The child receives injuries or bruises as a result.
- The length of punishment surpasses the child’s endurance.
Maltreatment
Under New York State Social Services Law, Section 412, a child is maltreated when:
- A parent or other person legally responsible for the child fails to provide the minimum degree of care and that failure results in impairment or imminent danger of impairment to the child’s physical, mental, or emotional condition, or
- A parent or other person legally responsible for the child causes a nonaccidental, serious physical injury to the child
It is important to note actual impairment or harm is not required. However, poverty in and of itself is not maltreatment.
Sexual Abuse/Exploitation
Sexual abuse includes situations in which the parent or another person who is legally responsible for a child who is younger than age 18 commits or allows sexual misconduct, rape or sexual abuse, commercial sexual exploitation, incest, production or possession of pornography, or sex trafficking. New York State Family Court Act, Section 1012(e)(iii), and Social Services Law, Section 371, list the following:
- Commits or allows to be committed any sex offense against the child, as defined in Article 130 of the penal law, including sexual misconduct, rape, and sexual abuse
- Allows, permits, or encourages the child to engage in child prostitution, as described in §§ 230.25, 230.30, and 230.32 of the penal law
- Commits an act of incest, as described in §§ 255.25, 255.26, and 255.27 of the penal law
- Allows the child to engage in acts or conduct to produce, promote, or possess child pornography, as described in Article 263 of the penal law
- Permits or encourages the child to engage in any act or commits or allows to be committed against the child any offense that would render the child either a victim of sex trafficking or a victim of severe forms of trafficking in persons pursuant to 22 U.S.C. § 7102
(CWIG, 2022)
Emotional Abuse
Emotional abuse is defined in New York State Family Court Act, Section 1012(h):
“Impairment of emotional health” and “impairment of mental or emotional condition” including a state of substantially diminished psychological or intellectual functioning in relation to, but not limited to, such factors as failure to thrive, control of aggressive or self-destructive impulses, ability to think and reason, acting out, or misbehavior, including incorrigibility, ungovernability, or habitual truancy; provided, however, that such impairment must be clearly attributable to the unwillingness or inability of the respondent to exercise a minimum degree of care toward the child.
Abandonment
The New York State Social Service Law, Section 384B, defines abandonment as a situation in which:
A parent evinces an intent to forgo his or her parental rights and obligations as manifested by his or her failure to visit the child and communicate with the child or agency, although able to do so and not prevented or discouraged from doing so by the agency. In the absence of evidence to the contrary, such ability to visit and communicate shall be presumed.
ABANDONED INFANT PROTECTION ACT
In 2000, New York State became one of the first states to enact a “safe-haven” law by passing the Abandoned Infant Protection Act (AIPA). The law designates specific locations as safe places for parents to relinquish their unharmed newborns. It helps ensure that unwanted infants are surrendered to persons who can provide immediate care for their safety and well-being. It also protects parents who feel that they have no choice other than abandonment and want to protect their child from harm.
Abandonment (discarding) of newborn infants in unsafe places is an example of extreme neglect. Under New York State Penal Law, Title O, Article 260, Section 260, it is considered a Class E felony and a Class A misdemeanor and must be reported by mandated reporters. Under the AIPA, amended in 2010, a parent will not be charged if the following criteria are met:
- The abandoned infant can be no more than 30 days old.
- The person abandoning the infant must have intended that the infant will be safe from physical injury and cared for appropriately.
- The person leaves the infant with an appropriate person or leaves the baby in a suitable location such as hospitals, police stations, nonprofit community health centers, health departments, and fire departments. The person immediately notifies an appropriate person of the infant’s location.
- The person must intend to wholly abandon the infant by relinquishing responsibility for and rights to the care and custody of the infant.
Any mandated reporter who learns of abandonment is obligated to fulfill mandated reporter responsibilities (see “Reporting Child Maltreatment/Abuse” later in this course). Even if the reporter is unsure of the name of the person abandoning the child, they must make a report, simply listing the unknown person as “Unknown” (NYS OCFS, n.d.-d).
CHILD ABUSE VICTIM DEMOGRAPHICS
Nationally in 2021 an estimated 600,000 children were victims of abuse and neglect. The actual number of victims could be higher because of the COVID-19 pandemic in 2021.
- 15% of all victims were in their first year of life.
- 28% of child maltreatment victims were under 2 years of age.
- The victimization rate of girls was 8.7 per 1,000 and of boys was 7.5 per 1,000.
- Native American or Alaska Native children had the highest rate at 15.2 per 1,000 children of the same race or ethnicity, and African American children had the second highest rate at 13.1 per 1,000 children of the same race or ethnicity.
- 76% of victims were neglected, 16% were physically abused, 10% were sexually abused, and 0.2% were victims of sex trafficking.
In 2021, it is estimated that 1,820 children died in the United States as the result of abuse or neglect. Boys had a fatality rate of 3.01 and girls had a rate of 2.15 per 100,000. Fatality rates were 5.6 per 100,000 for African American children, 1.94 for white children, and 1.44 for Hispanic children. This disproportionality may be due to a variety of complex factors and reflect larger societal dynamics (National Children’s Alliance, 2024).
In New York State in 2022:
- There were 5,058 documented victims of abuse or neglect, which represents a rate of 12.5 per 1,000 children and a 27% decrease from the rate of 16.9 per 1,000 children recorded in 2018.
- There were 2,677 recorded cases of medical neglect, 48,806 incidents of neglect, 4,715 cases of physical abuse, 2,161 cases of sexual abuse, and 433 cases of psychological maltreatment recorded.
(U.S. DHHS, 2024)
INDICATORS OF CHILD MALTREATMENT AND ABUSE
There are many possible indicators of child maltreatment or abuse, and these indicators should be viewed together, not in isolation. Similarly, each indicator must be considered in relation to the child’s current age and circumstances and in the context of their physical condition or behavior. These indicators are not all inclusive, and some children may not demonstrate signs or symptoms of abuse or neglect.
Another important aspect to assessing for possible abuse is obtaining an explanation for the presenting concern and whether that explanation is consistent with the observed physical and behavioral indicators. Abuse or maltreatment should never be assumed.
The mandated reporter is encouraged to consider any prior experiences with the child and possible differences between past and present observations.
Any assessment must be objective and free from implicit or explicit bias.
Physical Indicators
Healthcare professionals must be alert for physical injuries that are unexplained or inconsistent with the parent or other caretaker’s explanation or the developmental state of the child. However, it is important to remember that indicators of maltreatment or abuse may not always be of a physical nature or visible to view.
BRUISING
Bruising is the most common indicator of physical child abuse, and attention to bruises can be an important factor in identifying children who are at risk of physical abuse. It is important to know both normal and suspicious bruising patterns when assessing children’s injuries. Normal bruising usually occurs in the front of the body over bony areas such as the forehead, knees, shins, and elbows.
The TEN-4-FACESp validated clinical screening tool, developed by Dr. Mary Clyde Pierce, can be used to evaluate bruises in children under 4 years of age. The tool guides the clinician to assess bruising associated with three components (regions, infants, patterns) if there is no reasonable explanation for a bruise (Pierce et al., 2021). Children who are under 4 years should not have any bruises in the areas indicated in the chart below, and infants under 4 months should have no bruises anywhere. The size of the bruise is not as important as the location.
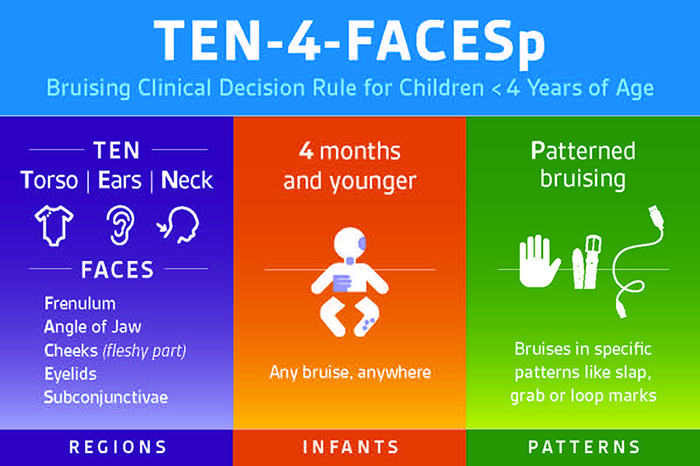
(Source: © Ann and Robert H. Lurie Children’s Hospital of Chicago.)

This pattern signals the blow of a hand to the face of a child. (Source: Research Foundation of SUNY, 2011.)

Regular patterns reveal that a looped cord was used to inflict injury on this child. (Source: Research Foundation of SUNY, 2011.)
LACERATIONS OR ABRASIONS
Typical indications of unexplained lacerations and abrasions that are suspicious include:
- On the face, lips, or mouth
- To external genitalia
BURNS
Unexplained burns include:
- Cigar or cigarette burns, especially on soles, palms, back, or buttocks
- Immersion burns by scalding water (sock-like, glove-like, doughnut-shaped on buttocks or genitalia; “dunking syndrome”)
- Patterned like an electric burner, iron, curling iron, or other household appliance
- Rope burns on arms, legs, neck, or torso

A steam iron was used to inflict injury on this child. (Source: Research Foundation of SUNY, 2011.)
FRACTURES
Unexplained fractures may include:
- Fractures to the skull, nose, or facial structure
- Multiple or spiral fractures
- Fractures in various stages of healing
(SD DSS, 2020)
HEAD INJURIES
Typical indications of unexplained head injuries include:
- Absence of hair or hemorrhaging beneath the scalp due to vigorous hair pulling
- Subdural hematoma (a hemorrhage beneath the outer covering of the brain, due to severe hitting or shaking)
- Retinal hemorrhage or detachment, due to shaking
- Whiplash or pediatric abusive head trauma
- Eye injury
- Jaw and nasal fractures
- Tooth or frenulum (of the tongue or lips) injury
PHYSICAL NEGLECT
Indicators of physical neglect include:
- Consistent hunger
- Poor hygiene (skin, teeth, ears, etc.)
- Inappropriate attire for the season
- Failure to thrive (physically or emotionally)
- Positive indication of toxic exposure, especially in newborns, such as drug withdrawal symptoms, tremors, etc.
- Delayed physical development
- Speech disorders
- Consistent lack of supervision, especially in dangerous activities or for long periods of time
- Unattended physical problems or medical or dental needs
- Chronic truancy
- Abandonment
Behavioral Indicators
Careful assessment of a child’s behavior may also indicate physical abuse, even in the absence of obvious physical injury. Behavioral indicators of physical abuse include the following:
- Withdrawal from friends or usual activities
- Changes in behavior (e.g., aggression, anger, hostility, or hyperactivity)
- Changes in school performance
- Depression, anxiety or unusual fears, or a sudden loss of self-confidence
- An apparent lack of supervision
- Frequent absences from school
- Reluctance to leave school activities, as if not wanting to go home
- Attempts at running away
- Rebellious or defiant behavior
- Self-harm or attempts at suicide
(Mayo Clinic, 2018; NYS OCFS, n.d.-c)
A child may demonstrate behavioral indicators of neglect such as:
- Begging or stealing food
- Extended stays at school (early arrival or late departure)
- Constant fatigue, listlessness, or falling asleep in class
- Alcohol or other substance abuse
- Delinquency, such as shoplifting
- Reports there is no caretaker at home
- Runaway behavior
- Habit disorders (sucking, nail biting, rocking, etc.)
- Conduct disorders (antisocial or destructive behaviors)
- Neurotic traits (sleep disorders, inhibition of play)
- Psychoneurotic reactions (hysteria, obsessive-compulsive behaviors, phobias, hypochondria)
- Extreme behavior (compliant or passive, aggressive or demanding)
- Overly adaptive behavior (inappropriately adult, inappropriately infantile)
- Delays in mental or emotional development
- Suicide attempt
(Clermont County CPS, 2021; NYS OCFS, n.d.-c)
ASSESSING FOR EDUCATIONAL NEGLECT
Poor school attendance, in and of itself, does not equate to a reasonable cause to suspect maltreatment, and a report of suspected educational neglect should be called in to the SCR only as a last resort. School personnel should first try working with the student, family, and community agencies to identify needs and resources available to meet those needs.
All of the following elements must be present to warrant a call to the SCR for educational neglect:
- The child must be of compulsory school age and currently living in New York State.
- The child must be excessively absent without a valid reason or excuse.
- The child’s education must be impaired due to the excessive absenteeism (or the child has an Individualized Education Program [IEP] and has missed necessary services due to excessive absenteeism).
- The parent or PLR has been made aware of the excessive absenteeism and impairment by means beyond simply sending a note home or leaving a voicemail message.
- School officials have made efforts to engage the child and parent or PLR.
- No parent or PLR has taken any action to rectify the situation.
(NYS OCFS, 2025)
Indicators of Sexual Abuse
Child sexual abuse involves the coercion of a dependent, developmentally immature person to commit a sexual act with someone older. For example, an adult may sexually abuse a child or adolescent, or an older child or adolescent may abuse a younger child. A perpetrator does not have to be an adult in order to sexually abuse a child (RAINN, 2021).
The fact that sexual abuse may be carried out by a family member or friend further increases the child’s reluctance to disclose the abuse, as does shame and guilt plus the fear of not being believed. The child may fear being hurt or even killed for telling the truth and may keep the abuse secret rather than risk the consequences of disclosure. Very young children may not have sufficient language skills or vocabulary to describe what happened (Clermont County CPS, 2021; RAINN, 2021).
Child sexual abuse is found in every race, culture, and class throughout society. Girls are sexually abused more often than boys; however, this may be due to boys’—and later, men’s—tendency not to report their victimization.
Most perpetrators of child sexual abuse are people who are known to the victim. As many as 93% of children who are sexually abused under the age of 18 know the abuser. There is no particular profile of a child molester or of the typical victim. Even someone highly respected in the community—the parish priest, a teacher, or coach—may be guilty of child sexual abuse. Anyone, including parents, can be a perpetrator, and most are male.
Negative effects of sexual abuse vary from person to person and range from mild to severe in both the short and long term. Victims may exhibit anxiety, difficulty concentrating, and depression. They may develop eating disorders, self-injury behaviors, substance abuse, or suicide. The effects of childhood sexual abuse often persist into adulthood (Clermont County CPS, 2021; RAINN, 2021).
PHYSICAL INDICATORS OF SEXUAL ABUSE
Physical evidence of sexual abuse may not be present or may be overlooked. Victims of child sexual abuse are seldom injured due to the nature of the acts. Most perpetrators of child sexual abuse go to great lengths to “groom” the children by rewarding them with gifts and attention and try to avoid causing them pain in order to ensure that the relationship will continue.
If physical indicators occur, they may include:
- Symptoms of sexually transmitted diseases, including oral infections, especially in preteens
- Difficulty in walking or sitting
- Torn, stained, or bloody underwear
- Pain, itching, bruising, or bleeding in the genital or anal area
- Bruises to the hard or soft palate
- Pregnancy, especially in early adolescence
- Painful discharge of urine or repeated urinary infections
- Foreign bodies in the vagina or rectum
- Painful bowel movements
(Clermont County CPS, 2021; RAINN, 2021; NYS OCFS, n.d.-c)
BEHAVIORAL INDICATORS OF SEXUAL ABUSE
Children’s behavioral indicators of child sexual abuse include:
- Unwillingness to change clothes for or participate in physical education activities
- Withdrawal, fantasy, or regressive behavior, such as returning to bedwetting or thumb-sucking
- Inappropriate, bizarre, suggestive, or promiscuous sexual behavior
- Inappropriate sexual knowledge for age
- Verbal disclosure of sexual assault
- Involvement in commercial sexual exploitation
- Forcing sexual acts on other children
- Extreme fear of closeness or physical examination
- Suicide attempts or other self-injurious behaviors
- Layered or inappropriate clothing
- Hiding clothing
- Lack of interest or involvement in activities
(Clermont County CPS, 2021; RAINN, 2021; NYS OCFS, n.d.-c)
SEX TRAFFICKING / COMMERCIAL SEXUAL EXPLOITATION OF CHILDREN
The crime of sex trafficking of children is a type of child abuse increasingly encountered in the healthcare setting. It is defined in the Trafficking Victims Protection Act (18 USC §1591) as “to recruit, entice, harbor, transport, provide, obtain, or maintain by any means a person, or to benefit financially from such action, knowing or in reckless disregard that the person has not attained the age of 18 years and will be caused to engage in a commercial sex act.”
Victims of sex trafficking seldom self-disclose, and many will resist disclosure because they have been threatened or feel shame, guilt, or loyalty to the trafficker. Some youth do not self-identify as victims. It is important for healthcare providers to ask about exploitation because 88% of adolescent victims of trafficking reported an encounter with a healthcare provider during the time that they were being exploited.
Indicators in Children with Intellectual and Developmental Disabilities
The rate of child abuse and neglect is at least three times higher in children with disabilities than in the typically developing population. Children with disabilities were found to be re-referred to CPS more frequently and to have been abused more frequently (Legano et al., 2021). Therefore, mandated reporters must be aware of indicators of abuse or maltreatment in children with intellectual or developmental disabilities (I/DD).
The New York Commissioner of Education defines intellectual disability as “significantly subaverage general intellectual functioning, existing concurrently with deficits in adaptive behavior and manifested during the developmental period, that adversely affects a student's educational performance” (8NYCRR, part 200, section 200.1).
According to the New York State Mental Hygiene Law, Section 1.03(22), developmental disability means a disability of a person which:
Physical indicators of potential child maltreatment and abuse in children with I/DD may include:
- Unexplained injuries
- Poor hygiene
- Malnutrition or dehydration
- Medical neglect
- Physical restraint marks
Behavioral indicators may include:
- Sudden or gradual changes in behavior
- Regression in previously acquired skills
- Self-harming
- Signs of agitation, anxiety or stress around particular caregivers
- Inappropriate sexual behavior
- Changes in sleep pattern
Children with I/DD may also display communication changes due to maltreatment or abuse, such as:
- Difficulty communicating
- Changes in vocalization
- Nonverbal cues
Mandated reporters may also observe behavioral indicators in caregivers to children with I/DD, such as:
- Inconsistent explanations
- Dismissive attitude
- Excessive anger or frustration
- Isolation from support networks
(NYS OCFS, 2025)
CASE
SCENARIO
Esmerelda, a school teacher, stops by her friend Janie’s house for coffee. While she is there, Janie’s son, Caden, who is a student in Esmerelda’s class, runs into the kitchen and for no apparent reason aggressively shoves his 2-year-old sister, who falls to the floor. Caden, age 7, has been diagnosed with a spectrum disorder. While the toddler is not injured, Janie yells angrily at Caden, picks him up, and throws him across the kitchen, where he slides into a cabinet, hitting the back of his head.
Esmerelda is surprised by her friend’s excessive anger and acknowledges how frightening and stressful it must be for Janie to have a child with a developmental disability. She also understands that such behavior by a caregiver may be associated with maltreatment of such a child. Esmeralda examines Caden and finds that he is okay.
Esmerelda is aware that she is a mandated reporter of child abuse because she is a teacher who has responsibility for her students. She also has reasonable cause to suspect that Caden may be a victim of child abuse due to the severity of the incident that she observed. Esmerelda lets Janie know that she must make an immediate report of suspected child abuse.
Esmerelda also expresses her concern for the family. She asks Janie if she can refer Caden to a program for children with learning differences that is provided by the school district. Janie tearfully agrees, and Esmerelda makes a call to the school district to gather information about the program. When calling in her report by phone, Esmerelda describes the incident, including Janie’s desire to help her child and her voluntary interest in a referral to services that can help her.
Esmerelda makes a point to call Janie the next day and frequently thereafter. Two months later, Janie tells Esmerelda that a social worker helped her find a program in which she is learning appropriate new ways of dealing with the challenge of Caden’s learning differences.
Indicators in a Virtual Environment
Mandated reporters must be aware of indicators of abuse or maltreatment that can be assessed for in a virtual environment for such children who attend school remotely, visit doctors using telemedicine, or participate in therapy sessions on virtual platforms.
Recommendations for assessing for potential abuse or maltreatment when interacting in a virtual environment include:
- Use reliable technology with adequate lighting and sound.
- Confirm the child’s physical location in the event you need to contact emergency services.
- Provide clear channels to reach out, such as email, phone, chat, text, or online tools.
- Make sure the child is present for at least part of the virtual interaction.
- Be alert if a child turns off a webcam or is very hesitant to use one.
- Ask everyone to introduce themselves who is in the room with the child or who enters the room after the visit starts.
- Be alert for indications that a child is trying to communicate something without someone else in the room noticing.
- Pay attention to nonverbal cues (e.g., if a child’s demeanor or behavior is different when someone else enters the room).
- Listen for concerning statements a child makes, including to siblings or peers.
- Be alert for altercations between children or adults. (Even if altercations do not rise to a level of suspected abuse, they may create an opportunity for a conversation about safety or managing stress.)
- Observe the child’s body for possible physical indicators, even if only the face, neck, shoulders, or chest may be visible.
- Note behavior in the child that indicates depression or anxiety.
- Ask if there is enough privacy for the child or parent to discuss sensitive matters. This may mean asking nonparticipating household members to move to a different room.
- Assess the environment (e.g., Are there noticeable unsafe conditions? Is there appropriate supervision for the child? Are young children watching even younger siblings?)
- Watch carefully, verbalize one’s observations, and ask if the family agrees.
(NYS OCFS, 2025)
Risk Factors for Perpetrating Child Abuse
A caregiver may have certain characteristics that increase the likelihood that they may become a perpetrator of child abuse or neglect. When health professionals observe indicators of possible abuse, they should consider whether the presence of risk factors in a caregiver may signal a need to examine the situation more carefully.
Individual risk factors include:
- Caregivers with drug or alcohol issues
- Caregivers with mental health issues, including depression
- Caregivers who don't understand children's needs or development
- Caregivers who were abused or neglected as children
- Caregivers who are young or single parents or parents with many children
- Caregivers with low education or income
- Caregivers experiencing high levels of parenting stress or economic stress
- Caregivers who use spanking and other forms of corporal punishment for discipline
- Caregivers in the home who are not a biological parent
- Caregivers with attitudes accepting of or justifying violence or aggression
Relationship/family risk factors include:
- Families that have household members in jail or prison
- Families that are isolated from and not connected to other people (extended family, friends, neighbors)
- Families experiencing other types of violence, including relationship violence
- Families with high conflict and negative communication styles
Community risk factors include:
- Communities with high rates of violence and crime
- Communities with high rates of poverty and limited educational and economic opportunities
- Communities with high unemployment rates
- Communities with easy access to drugs and alcohol
- Communities where neighbors don't know or look out for each other
- Communities where there is low community involvement among residents
- Communities with few community activities for young people
- Communities with unstable housing and where residents move frequently
- Communities where families frequently experience food insecurity
(CDC, 2024)
Nationally, the most common risk factors reported with child maltreatment are substance abuse and domestic violence (U.S. DHHS, 2024).
REPORTING CHILD ABUSE, MALTREATMENT, AND NEGLECT
[Information in this section is taken from NYC ACS (2021) and New York State Office of Children and Family Services (2024).]
Anyone may report suspected child abuse at any time and is encouraged to do so. All reports are confidential and may be made anonymously by members of the public.
Who Must Report Abuse?
Mandated reporters are individuals required by law to call the Statewide Central Register of Child Abuse and Maltreatment (SCR) when, in their professional role, they develop a reasonable cause to suspect a child under the age of 18 is being maltreated or abused by a parent or person over the age of 18 who is legally responsible for the care of the child at the relevant time.
What Situations Require That a Report Be Made?
New York State law requires mandated reporters to report suspected child abuse or maltreatment in the following three situations:
- When a mandated reporter has reasonable cause to suspect that a child whom the reporter sees in their professional or official capacity is abused or maltreated.
- When a mandated reporter has reasonable cause to suspect that a child is abused or maltreated where the parent or person legally responsible for such child comes before them in their professional or official capacity and states from personal knowledge facts, conditions, or circumstances which, if correct, would render the child abused or maltreated.
- Whenever a mandated reporter suspects child abuse or maltreatment while acting in their professional capacity as a staff member of a medical or other public or private institution, school, facility, or agency, they shall immediately notify the person in charge of that school, facility, institution, or their designated agent that a report has been made. The person in charge of the institution will then (also) become responsible for reporting or causing a child abuse report to be made to the county Child Protective Services (CPS) agency.
Mandated reporters can be held liable by both the civil and criminal legal systems for intentionally failing to make a report of suspected abuse that was encountered while acting in their professional capacity. (See also “Consequences for Failing to Report” below.)
REASONABLE CAUSE
There can be “reasonable cause” to suspect that a child is abused or maltreated if, considering the physical evidence observed or told about, and based on the reporter’s own training and experience, it is possible that the injury or condition was caused by neglect or by nonaccidental means. Poverty in and of itself does not equate to maltreatment or abuse.
Certainty is not required. The reporter need not be certain that the injury or condition was caused by neglect or by nonaccidental means. The reporter need only be able to entertain the possibility that it could have been neglect or nonaccidental in order to possess the necessary “reasonable cause.” It is enough for the mandated reporter to distrust or doubt what is personally observed or told about the injury or condition.
In child abuse cases, many factors can and should be considered in the formation of that doubt or distrust. Physical and behavioral indicators may also help form a reasonable basis of suspicion. Although these indicators are not diagnostic criteria of child abuse, neglect, or maltreatment, they illustrate important patterns that may be recorded in the written report when relevant.
When Must a Report Be Made?
The law requires that mandated reporters must “personally make a report to the Statewide Central Register of Child Abuse and Maltreatment (SCR)” and “immediately notify the person in charge of the institution, school, facility, or agency where they work or the designated agent of the person in charge that a report has been made.”
In the case of suspected child abuse, maltreatment, or neglect, mandated reporters are required to make an oral telephone report immediately at any time of day, seven days a week. In addition, a written report must be filed within 48 hours of the oral report.
- Mandated reporters should make an oral telephone report to the Statewide Central Register of Child Abuse and Maltreatment (SCR) by calling the statewide, toll-free mandated reporter hotline at 800-635-1522 or 311 in New York City. (The general public can call 311 in New York City or call the SCR directly at 800-342-3720.)
- A written report on Form LDSS-2221A, signed by the reporter, must be filed within 48 hours of the oral report with the local Department of Social Services (LDSS) assigned the investigation. Mandated reporters can request the mailing address of the local agency when making the oral report to the hotline. (A written report involving a child cared for away from the home [e.g., foster care, residential care] should be submitted to the New York State Child Abuse and Maltreatment Register, P.O. Box 4480, Albany, NY 12204-0480.) Written reports are admissible as evidence in any judicial proceedings; accurate completion is vital.
(See also “Resources” at the end of this course.)
What Is Included in the Report?
At the time of an oral telephone report, the Child Protective Services (CPS) specialist will request the following information:
- How the child has been affected
- Names and addresses of the child and parents or other person responsible for care
- Location of the child at the time of the report
- Child’s age, gender, and race
- Nature and extent of the child’s injuries, abuse, or maltreatment, including any evidence of prior injuries, abuse, or maltreatment to the child or their siblings
- Name of the person or persons suspected to be responsible for causing the injury, abuse, or maltreatment (“subject of the report”)
- Family composition
- Any special needs or medications
- Whether an interpreter is needed
- Source of the report
- Person making the report and where reachable
- Actions taken by the reporting party, including taking of photographs or X-rays, removal or keeping of the child, or notifying the medical examiner or coroner
- Any personal safety issues that may impact CPS worker investigations (e.g., weapons, dogs)
- Any additional information that may be helpful
A reporter is not required to know all of the above information in making a report; therefore, lack of complete information does not prohibit a person from reporting. However, information necessary to locate a child is crucial.
SUBJECT OF THE REPORT
For purposes of reporting suspected cases of child abuse and maltreatment to the Statewide Central Register of Child Abuse and Maltreatment and Child Protective Services, it is important to understand the definition of who can be the “subject of the report” as defined by Section 412.4 of the Social Services Law.
- “Subject of the report” means any parent, guardian, custodian, or other person 18 years of age or older who is legally responsible for a child and who is allegedly responsible for causing—or allowing the infliction of—injury, abuse, or maltreatment to such child.
- “Subject of the report” also means an operator of or employee or volunteer in a home operated or supervised by an authorized agency, the Division for Youth, or an office of the Department of Mental Hygiene, or a family daycare home, daycare center, group family daycare home, or a day-services program who is allegedly responsible for causing—or allowing the infliction of—injury, abuse, or maltreatment to a child.
What Happens Once a Report Is Made?
The CPS unit of the local Department of Social Services is required to begin an investigation of each report within 24 hours. The investigation includes an evaluation of the safety of the child named in the report and any other children in the home and a determination of risk to the children if they continue to remain in the home.
If the Department records indicate a previous report concerning a “subject of the report,” other persons named in the report, or other pertinent information, the appropriate agency or local CPS must be immediately notified of this fact.
What Follow-Up Can Be Made by the Reporter?
Section 422.4 of the Social Services Law provides that a mandated reporter can receive, upon request, the findings of an investigation made pursuant to their report. This request can be made to the SCR at the time of making the report or to the appropriate local CPS at any time thereafter. However, no information can be released unless the reporter’s identity is confirmed.
If the request for information is made prior to the completion of an investigation of a report, the released information shall be limited to whether the report is “indicated” (i.e., substantiated), “unfounded,” or “under investigation,” whichever the case may be.
If the request for information is made after the completion of an investigation of a report, the released information shall be limited to whether a report is “indicated” or, if the report has been expunged, that there is “no record of such report,” whichever the case may be.
REPORTING AND HIPAA PROVISIONS
The Health Insurance Portability and Accountability Act of 1996 (HIPAA) contains privacy provisions that have caused confusion regarding the obligation of a mandated reporter to provide copies of written records that underlie the report. However, these HIPAA provisions do not affect the responsibilities of mandated reporters as they are defined in New York Social Services Law.
Consequences for Failing to Report
Any person, official, or institution required to report a case of suspected child abuse or maltreatment that willfully fails to do so:
- Can be charged with a Class A misdemeanor and subject to criminal penalties
- Can be sued in a civil court for monetary damages for any harm caused by such failure to report to the SCR
Failure to report also leads to broader repercussions. CPS cannot act until child abuse is identified and reported—that is, services cannot be offered to the family nor can the child be protected from further suffering (NYS OCFS, 2024).
Liability and Immunity
To encourage prompt and complete reporting of suspected child abuse and maltreatment, Social Services Law, Section 419, affords the reporter certain legal protections from liability. Any persons, officials, or institutions that in good faith make a report, take photographs, or take protective custody of a child or children have immunity from any liability, civil or criminal, that might result from such actions.
All persons, officials, or institutions who are required to report suspected child abuse or maltreatment are presumed to have done so in good faith as long as they were active in the discharge of their official duties and within the scope of their employment and so long as their actions did not result from willful misconduct or gross negligence (NYS OCFS, 2024).
Confidentiality
The Commissioner of Social Services and the local Department of Social Services are not permitted to release to the subject of a report any data that identifies the person who made the report unless that person has given written permission for the SCR to do so. The person who made the report may also grant the local CPS permission to release their identity to the subject of the report. If a reporter needs reassurance, they should feel free to emphasize the need for confidentiality if the situation warrants (NYS OCFS, 2024).
CONCLUSION
Child abuse, maltreatment, and neglect negatively impact the health and well-being of the people of New York. Child victimization is not only a social problem but also a serious public health issue. Child abuse and neglect affect not only the victims while they are children but also shape the adults these children will become. The fundamental goal is to prevent child abuse and neglect from occurring at all in order to create healthy children who will in turn become healthy adults.
Mandated reporters are obligated to report suspected child abuse, neglect, and maltreatment. Reporting suspected child abuse is their duty as professionals, but it is also an opportunity to help improve the health and well-being of children and take part in creating a healthier society.
RESOURCES
Adverse childhood experiences (ACEs) (Office of Children and Family Services)
Child Abuse Hotline
800-342-3720 (general public)
800-635-1522 (mandated reporters)
311 (in New York City)
Child Protective Services FAQ (Office of Children and Family Services)
HEARS Family Line (Help, Empower, Advocate, Reassure, and Support)
(888) 55-HEARS (554-3277)
Mandated Reporter Resource Center
New York State Trauma-Informed Network
Summary Guide for Mandated Reporters (NYS OCFS)
National
American Professional Society on the Abuse of Children
Child Welfare Information Gateway
Council on Child Abuse and Neglect (American Academy of Pediatrics)
REFERENCES
NOTE: Complete URLs for references retrieved from online sources are provided in the PDF of this course.
Centers for Disease Control and Prevention (CDC). (2024). Child abuse and neglect prevention: Risk and protective factors. https://www.cdc.gov
Child Welfare Information Gateway (CWIG). (2022). Definitions of child abuse and neglect: New York State. https://www.childwelfare.gov
Clermont County Children’s Protective Services (CPS). (2021). Detecting child abuse and neglect. http://cps.clermontcountyohio.gov
Human Trafficking Collaborative (HTC), University of Michigan. (n.d.). Trauma-informed care. https://humantrafficking.umich.edu
Legano LA, Desch LW, Messner SA, Idzerda S, et al. (2021). Maltreatment of children with disabilities. Pediatrics, 147(5), e2021050920. https://doi.org/10.1542/peds.2021-050920
Maryville University. (n.d.). How to identify and overcome your implicit bias. https://online.maryville.edu
Massachusetts Adult Education Professional Development (MAEPD) System. (n.d.). Project implicit: Harvard University’s implicit association test. https://www.sabes.org
Mayo Clinic. (2018). Child abuse. https://www.mayoclinic.org
National Center for Cultural Competence (NCCC). (n.d.). Two types of bias. https://nccc.georgetown.edu
National Children’s Alliance. (2024). National statistics on child abuse. https://www.nationalchildrensalliance.org
National Institutes of Health (NIH). (2022). Implicit bias. https://diversity.nih.gov
New York City Administration for Children’s Services (NYC ACS). (2021). How to make a report. https://www1.nyc.gov
New York State Office of Children and Family Services (NYS OCFS). (2025). 2025 NYS mandated reporter training syllabus.
New York State Office of Children and Family Services (NYS OCFS). (2024). Summary guide for mandated reporters in New York State. https://ocfs.ny.gov
New York State Office of Children and Family Services (NYS OCFS). (n.d.-a). Child protective services. https://ocfs.ny.gov
New York State Office of Children and Family Services (NYS OCFS). (n.d.-b). Adverse childhood experiences (ACEs). https://ocfs.ny.gov
New York State Office of Children and Family Services (NYS OCFS). (n.d.-c). Signs of child abuse or maltreatment. https://ocfs.ny.gov
New York State Office of Children and Family Services (NYS OCFS). (n.d.-d). Abandoned infant protection act. https://ocfs.ny.gov
Pierce MC, Kaczor K, Lorenz DJ, et al. (2021). Validation of a clinical decision rule to predict abuse in young children based on bruising characteristics. JAMA Network Open, 4(4), Article e215832. https://doi.org/10.1001/jamanetworkopen.2021.5832
Practical Psychology. (2022). Implicit association test. https://practicalpie.com
Rape, Abuse & Incest National Network (RAINN). (2021). Child sexual abuse. https://www.rainn.org
Research Foundation of SUNY/Center for Development of Human Services. (2011). Mandated reporter training: Identifying and reporting child abuse and maltreatment/neglect. Author.
South Dakota Department of Social Services (SD DSS). (2020). Signs of child abuse and neglect. https://dss.sd.gov
U.S. Department of Health & Human Services (U.S. DHHS), Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2024). Child maltreatment 2022. https://www.acf.hhs.gov
University College Cork (UCC). (2022). Implicit bias. https://www.ucc.ie/en/edi/hub/implicitbias/

Customer Rating
4.9 / 1514 ratings