Obesity in America
Management and Treatment in Children, Adolescents, and Adults
Online Continuing Education Course

Course Description
The United States is in an obesity epidemic. This course focuses on prevention for overweight and obesity. Often, the disease starts in childhood, continues through adolescence, and remains prevalent in adulthood. This continuing education course highlights the comorbidities and consequences and explains the effects of anti-obesity stigma. Strategize with your patients to prevent, manage, and treat this condition successfully.
Note: This course is also available as part of a package. See Nursing CEU Bundle - 30 ANCC Hours
Course Price: $47.00
Contact Hours: 9
Pharmacotherapeutic Hours: 0.25
Course updated on
July 1, 2025
"This was extremely well presented, and I gained more understanding of the topic." - Elizabeth, RN in New Hampshire
"Great course! Information I can use both professionally and personally." - Patricia, OT in Missouri
"Excellent information for me to share in both my professional and personal life. Thank you!" - Rebecca, RN in California
"Thank you for presenting this material with such compassion and deep knowledge of the plight and physical challenges of obese patients." - Barbara, RN in North Carolina
Obesity in America
Management and Treatment in Adults, Children, and Adolescents
Copyright © 2025 Wild Iris Medical Education, Inc. All Rights Reserved.
LEARNING OUTCOME AND OBJECTIVES: Upon completion of this course, you will have increased your knowledge about obesity, including its prevalence, consequences, contributing factors, interventions, and approaches to prevention and treatment. Specific learning objectives to address potential knowledge gaps include:
- Describe the prevalence and impact of overweight and obesity in U.S. adults, children, and adolescents.
- Examine the pathogenesis and etiology of overweight and obesity.
- Discuss the comorbidities and consequences of obesity.
- Explain the psychosocial effects of stigma and weight bias.
- Describe components of assessment for overweight or obesity.
- Summarize strategies for management and treatment of overweight and obesity in adults, children, and adolescents.
- Discuss considerations in caring for the bariatric patient.
- Outline ways to prevent overweight and obesity in all age groups.
TABLE OF CONTENTS
- Introduction
- What Causes Obesity?
- Comorbities and Consequences of Obesity
- Assessing for Overweight and Obesity
- Management and Treatment of Obesity in Adults
- Management and Treatment of Obesity in Children and Adolescents
- Caring for the Bariatric Patient
- General Strategies for Overweight and Obesity Prevention and Advocacy
- Conclusion
- Resources
- References
INTRODUCTION
According to the World Health Organization, in 2022, 1 in 8 people in the world were living with obesity. Worldwide, adult obesity has more than doubled since 1990, and adolescent obesity has quadrupled. Once considered a problem only in high-income countries, middle-income countries now have among the highest prevalence of overweight and obesity worldwide. Obesity is now recognized as one of the most important public health problems facing the world today (WHO, 2024; World Obesity, 2024).
The fundamental basis for overweight and obesity is a chronic energy imbalance that results from consuming more calories (diet) and expending less energy (physical activity). The cause of obesity, however, is multifactorial and includes an obesogenic environment, psychosocial factors, and genetic variants.
At the same time, the lack of an effective health system response to identify excess weight gain and fat deposition in their early stages is aggravating the progression to obesity with profound social, economic, and health implications for individuals and communities (WHO, 2024).
Defining Obesity
Obesity is defined by the Obesity Medicine Association (2023b) as:
A chronic, relapsing, multifactorial, neurobehavioral disease, wherein an increase in body fat promotes adipose tissue dysfunction and abnormal fat mass physical forces (mechanical stressors and pressures), resulting in adverse metabolic, biomechanical, and psychosocial health consequences.
The American Medical Association considers obesity a disease with multiple pathophysiologic aspects requiring a range of interventions to advance obesity treatment and prevention. The recognition of obesity as a disease allows for research interventions to prevent obesity and implement evidence-based treatments for those affected by obesity (OMA, 2023b; ASMBS, 2024a).
A disease is defined as “any harmful deviation from the normal structural or functional state of an organism, generally associated with certain signs and symptoms and differing in nature from physical injury” (Scarpelli et al., 2025).
Some have countered classifying obesity as a disease by saying that obesity is a risk factor for disease but not a disease itself. By such reasoning, however, a condition such as hypertension should not be classified as a disease. Hypertension, however, is a cardiovascular disease, a chronic disease that can lead to other serious conditions.
Arguments made by those who consider obesity to be a disease include:
- Genes may play a role, as well as other diseases or disorders, such as hypothyroidism, Cushing’s disease, and polycystic ovarian syndrome.
- Taking certain medications for other health conditions can lead to weight gain (e.g., antidepressants).
- Each person has their own base metabolic rate, so for two people who are the same height and eat the same diet, one may have obesity while the other does not.
- Some aspects of obesity are preventable; however, it is known that some people may make appropriate changes in diet and exercise yet still be unable to lose significant amounts of weight.
- Obesity is a complex, multifactorial disease scientifically shown to be brought on and sustained by many factors both within and beyond the individual’s control.
Arguments made by those who do not consider obesity to be a disease include:
- There is a lack of diagnostic criteria. There are no characteristic or unique symptoms, and obesity does not always lead to the same body function impairments.
- There are no indexes and standards for obesity measurement; weighing more does not always mean obesity is present.
- Obesity affects the body in many ways and may increase risk of medical conditions such as heart disease and diabetes. However, not everyone with obesity develops health challenges or symptoms, and not everyone with health challenges has obesity.
- Defining obesity as a disease may foster a culture of personal irresponsibility.
(Silva, 2024)
DETERMINING OBESITY
Among several classifications and definitions for degrees of obesity, the following is widely used:
| Classification | Body Mass Index (BMI) (kg/m2) |
|---|---|
| (Hamdy, 2025) | |
| Overweight | 25–29.9 |
| Obesity class 1 | 30–34.9 |
| Obesity class 2 | 35–39.9 |
| Obesity class 3 (also called severe, extreme, or massive obesity) |
≥40 |
However, while BMI has been useful for assessing population-level trends, it is not necessarily an accurate measure of obesity at an individual level. It does not measure body fat directly and cannot distinguish between fat, muscle, and bone. (See also “Calculating Body Mass Index” later in this course.)
Dual-energy X-ray absorptiometry (DEXA) scans are a special type of X-ray that can estimate the amount of fat tissue a person has.
Bioelectric impedance analysis (BIA) is a measurement of impedance of the body to a small electric current. Fat, muscle, and bone have different conductive properties, allowing for estimation of body fat percentage.
MRI estimated volume rather than the mass of adipose is currently an accurate and viable approach for estimating intra-abdominal adipose tissue.
In adults, waist circumference or waist–hip ratio is independently associated with morbidity after adjustment for relative weight (Sampson, 2023).
Scope of the Problem
GLOBALLY
A 2024 report by the NCD Risk Factor Collaboration estimates that more than one billion people in the world are now living with obesity, nearly 880 million adults and 159 million children and adolescents ages 5–19 years (World Obesity, 2024). In 2024, American Samoa had the highest obesity rate globally (80.2%), and Ethiopia had the lowest (1%) (World Population Review, 2024).
IN AMERICA
CDC data show that adult obesity prevalence in America remains high. In 2023, at least 1 in 5 adults and 1 in 5 children and adolescents in each state were found to be living with obesity. The states with the highest rates of obesity included West Virginia (41.2%), Mississippi (40.1%), and Arkansas (40%). In 23 states, more than 1 in 3 adults has obesity (CDC, 2024a).
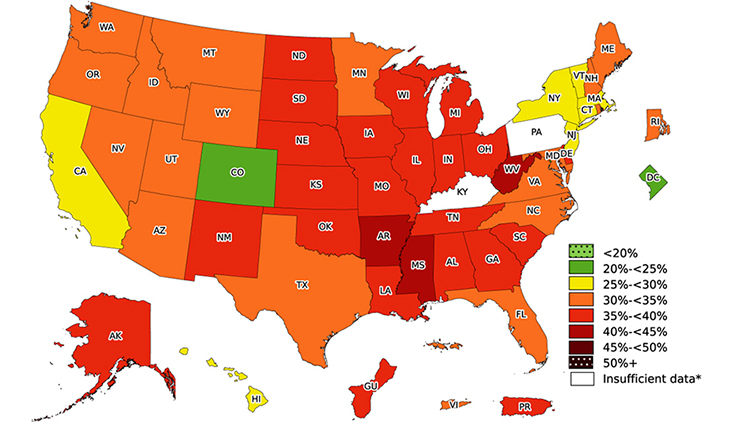
Prevalence of self-reported obesity among U.S. adults by state and territory, 2023. (Source: CDC, 2023a.)
Data from 2021 to 2023 indicates that obesity affects some population groups in the United States more than others:
- By race/ethnicity:
- Asian adults do not have an obesity prevalence at or above 35% in any state.
- In 16 states, White adults have an obesity prevalence at or above 35%.
- In 20 states, American Indian or Alaska Native adults have an obesity prevalence at or above 35%.
- In 34 states, Hispanic adults have an obesity prevalence at or above 35%.
- In 38 states, Black adults have an obesity prevalence at or above 35%.
- By age:
- Prevalence of obesity among adults was 40.3% in 2023.
- Prevalence of severe obesity in adults was 9.4% in 2023 and higher in adults ages 20–39 (9.5%) and 40–59 (12.0%) than in adults 60 and older (6.6%).
- In 2023, 1 in 5 American children were classified as having obesity:
- 12.7% among ages 2–5
- 20.7% among ages 6–11
- 22.2% among ages 12–19
- By sex:
- The prevalence of obesity was 39.2% in men and 41.2% in women. No significant differences between men and women were seen overall or in any age group.
- The prevalence of “severe” obesity in adults was 9.4% and was higher in women than men for each age group.
- Among men, prevalence was highest in those ages 40–59; among women, the prevalence was higher in those ages 20–39 and 40–59 than in those ages 60 and older.
- By educational level: Both men and women with college degrees had lower obesity prevalence compared with those who have less education.
- By income:
- Of those with incomes less than $15,000, 37.4% had obesity.
- Of those with an income of $75,000 or greater, 29.4% had obesity.
- Among non-Hispanic Black men, the obesity rate is higher in the highest income level.
- Among non-Hispanic White, Non-Hispanic Asian, and Hispanic women, obesity prevalence is lower in the highest income group compared to middle- and lower-income groups.
- Among non-Hispanic Black women, there was no significant difference in obesity prevalence based on income level.
(CDC, 2024a; Lyun et al., 2024)
ECONOMIC AND SOCIAL IMPACTS
The economic burden of obesity remains a paramount global concern due to its escalating prevalence, which imposes substantial pressures on healthcare systems, hampers productivity, and detracts from quality of life. Obesity has a strong impact on the global economy, with total costs estimated to range from 0.05% to 2.24% of a country’s gross domestic product. World Obesity (2024) estimates that the annual global economic impact of obesity will surpass $4 trillion by 2035. Studies to date have identified at least four major categories of economic impact linked to the problem of obesity: direct medical costs, productivity costs, transportation costs, and human capital costs.
Because obesity is linked with higher risk for health conditions such as hypertension, type 2 diabetes, hypercholesterolemia, coronary heart disease, stroke, asthma, and arthritis, direct medical spending on diagnosis and treatment of these conditions also increases with rising obesity levels. It has been estimated that in 2019 the annual medical cost of obesity was nearly $173 billion, with medical costs $1,861 higher for those with obesity compared to those at a healthy weight.
In addition to the direct medical costs, indirect costs include negative effects on productivity. The productivity costs of obesity are well-documented, with widespread agreement that such costs are substantial. Productivity costs are increased due to absenteeism for obesity-related reasons and decreased productivity of employees while at work.
Other categories of productivity costs include:
- Premature mortality and loss of quality-adjusted life years (QALYs)
- Higher rates of disability benefit payments
- Increase in disability insurance premiums
The cost of transportation is another economic issue of concern. Obesity requires larger vehicles and more fuel, leading to greater greenhouse gas emissions. The cost of airline fuel is also significant, with calculated weight gain shown to require approximately 350 million extra gallons of jet fuel in a year (Dietz, 2023a; Sweis, 2024). Beyond economic costs, obesity can lead to social stigma and discrimination in employment and social situations. Despite decades of research that demonstrate the dominant influence of genetic and environmental factors in the development of obesity, obesity continues to be viewed as a result of individual decision-making, leading to harmful assumptions about the lifestyles and characters of people with obesity (Westbury et al., 2023).
WHAT CAUSES OBESITY?
There are many factors involved in the etiology of obesity. These factors result in a chronic positive energy balance regulated by a complex interaction between endocrine tissues and the central nervous system. Possible components and contributors for the development of obesity include:
- Metabolic factors
- Genetic factors
- Level of activity
- Endocrine factors
- Race, sex, and age factors
- Ethnic and cultural factors
- Socioeconomic status
- Dietary habits
- Smoking cessation
- Pregnancy and menopause
- Psychological factors
- History of gestational diabetes
- Lactation history in mothers
- Gut microbiome characteristics
- Exposure to endocrine-disrupting chemicals in the environment and food supply
Studies suggest that the genetic contribution to adult obesity is 40%–70% in most individuals. If a young person has one biologic parent with obesity, the risk of obesity is increased three to four times compared with those who do not have a parent with obesity.
Rare forms of obesity result from certain genetic abnormalities, including:
- Prader-Willi Syndrome
- Bardet-Biedl syndrome
- Monogenic obesities:
- Melanocortin 4 receptor deficiency (the most common)
- Leptin and leptin receptor deficiency
- Proopiomelanocortin (PMC) deficiency
It is also believed that obesity has an infectious component, and several studies have linked obesity to infection with adenovirus 36 (ADV36). This adenovirus interferes with insulin resistance and cytokine production in individuals with obesity.
Individuals who are overweight or have obesity have altered circulatory levels of inflammatory cytokines such as interleukin (IL)-6, tumor necrosis factor (formerly referred to as TNF), C-reactive protein (CRP), and IL-18. Resistin and visfatin are suggested as important pro-inflammatory mediators that interfere with the regulation of insulin sensitivity (Perreault & Rosenbaum, 2024; Khanna et al., 2024; Hamdy, 2025; Sanches et al., 2023).
Excess Adipose Tissue
Obesity is characterized by the accumulation and inflammation of excessive body fat (adipose tissue). Adipose tissue is the primary storage site for excess energy and is classified as an endocrine gland that plays many roles in metabolism, including modulating energy expenditure, appetite, insulin sensitivity, bone metabolism, reproductive and endocrine functions, inflammation, and immunity.
Adipose tissue makes and releases the hormone leptin, which acts on the brainstem and hypothalamus to help inhibit hunger and regulate long-term balance between food intake and energy expenditure. Because the amount of leptin in the blood is directly proportional to the amount of adipose tissue, having excess adipose tissue results in high levels of leptin.
This leads to leptin resistance, wherein the brain no longer responds normally to leptin. Since the brain is constantly being stimulated by leptin, there is an absence of the sensation of feeling full, causing one to eat more even though the body has enough fat stores. The seeming lack of leptin also causes the body to enter starvation mode (adaptive thermogenesis) and to lower the basal metabolic rate in order to conserve energy, resulting in the use of fewer calories at rest and worsening weight gain (Cleveland Clinic, 2022a).
The distribution of adipose tissue in the body can vary depending on sex. In general, men accumulate fat around the waist, and women accumulate more fat around the hips. Geneticists have found distinct regions in the human genome that are associated with fat distribution, and knowledge of their precise functions could provide insights into the biologic mechanisms underlying obesity (Rogers, 2024).
Genetics
A growing body of evidence suggests that obesity is genetic. Between 200 and 500 specific genes have been linked to the disease, and twin studies have supported that hypothesis. Several measures of obesity show a high rate of heritability.
Studies of adiposity between twins, adoptees, and their parents, as well as within families, all suggest the existence of genetic factors in humans with obesity. The heritability of adiposity estimated from twin studies is high, ranging from 40% to 75%, with only slightly lower values in twins raised apart compared to those raised together. Responses to overfeeding and underfeeding, energy expenditure, food choices, hunger, and satiation have all been shown to be significantly heritable (Perreault & Rosenbaum, 2024).
Obesity is classified as either monogenetic, polygenetic, or syndromic based on its genetic contribution.
Monogenetic obesity involves rare mutations of one gene, typically causing severe early-onset obesity with abnormal feeding behavior and endocrine disorders.
Polygenetic (also known as common obesity) arises from interactions between multiple gene variants and elements in the environment that may facilitate development of obesity. Sixty percent of genetic cases fit into this category. Studies on polygenic obesity have found over 900 genetic variants associated with obesity.
Syndromic obesity is associated with intellectual disability, dysmorphic features, or abnormalities affecting different organs and systems. These include:
- Prader-Willi syndrome (PWS)
- Bardet-Biedl syndrome (BBS)
- Pseudohypoparathyroidism (PHP)
- Alström syndrome (ALMS)
- Beckwith-Wiedemann syndrome (BWS)
- Carpenter syndrome
- Cohen syndrome
- Down syndrome
(NIH, 2024a, NIH, 2024b; Kalinderi et al., 2024; NORD, 2023a, NORD 2023b)
Epigenetics and Obesogens
Epigenetics is the study of how environmental factors and behaviors can alter gene function. Epigenetic changes are reversible and do not change the sequence of DNA bases, but they can change how the body reads a DNA sequence and subsequently how proteins are produced. An environmental factor can result in an epigenetic change by adding a chemical (a methyl group) to DNA that turns genes off.
Obesogens are chemicals in common products that may contribute to obesity. Obesogens are endocrine disruptors that play a role in metabolism and that may affect human hormones, changing the way a body makes, stores, and uses fats. These chemicals do not directly cause obesity, but they may increase susceptibility to weight gain.
Research indicates that there are several ways obesogens affect the body, including:
- Increasing fat cells. In some instances, the new cells may be unusually large, allowing for more fat to build up in the body.
- Blocking fat burning so that fat cells cannot release stored fat.
- Altering appetites by affecting the hypothalamus, which releases hormones that signal hunger and others that signal satiety, leading to a tendency to compulsively eat and not stop even though the person is no longer hungry.
The most sensitive time for exposure to obesogens is during early development—as a fetus or during the first years of life—when the body’s weight-control mechanisms are being developed (Ratini, 2023; NIEHS, 2024a).
CHEMICAL OBESEGENS
- Flame retardants: used in many electronics, furniture, and building materials and linked to endocrine disruption and thyroid dysfunction
- Polychlorinated biphenyls (PCBs): present in products and materials produced before 1979 and linked to increased risk for cancer, infection, diabetes, heart attack and stroke, and difficulties with learning and memory
- Tobacco smoke, which contains a mix of more than 7,000 chemicals
- Outdoor air pollution
- Tributyltin (TBT), a pesticide additive, banned in 2008, due to possible harmful effects on the immune and neurological systems and embryos in mammals
- Phthalates: found in many consumer products and associated with increased risk of cancer, asthma and allergies, and learning attention and behavioral difficulties in children
- Bisphenol A (BPA): used primarily in the production of polycarbonate plastics and epoxy resins and linked to childhood obesity
- Many types of pesticides
Endocrine Diseases
Along with the hormones released from adipocytes, other hormones secreted by the endocrine system can be involved in conditions that result in obesity. These endocrine conditions can include:
- Hypothyroidism
- Polycystic ovarian syndrome
- Hyperandrogenism in females
- Cushing’s syndrome
- Hypothalamic disorders
- Hypogonadism in males
- Growth hormone deficiency
- Pseudohypoparathyroidism
The mechanisms for the development of obesity vary based on the endocrine condition. Hypothyroidism, for example, involves an accumulation of fluid-retaining hyaluronic acid, resulting in excess retention of salt and water, which is associated with changes in body weight and composition. It also affects body temperature, energy expenditure, food intake, and glucose and lipid metabolism (ATA, 2024).
Polycystic ovary syndrome (PCOS), the most common endocrine disorder in women, is marked by some combination of irregular periods, an excess of androgen, and polycystic ovaries (enlarged and lined with follicles). PCOS causes weight gain, and obesity can also exacerbate the effects of the condition (TGH, 2025).
Cushing’s syndrome occurs when the body has too much cortisol for a long period of time. This can be due to the body producing too much cortisol or from taking glucocorticoid medications. Most patients with Cushing’s syndrome have obesity due to stimulation of appetite and the effect of glucocorticoids to promote deposition of visceral fat (Mayo Clinic, 2023a).
Hypothalamic Obesity
Hypothalamic obesity specifically refers to excess weight gain that may follow malformation or anatomical injury to the hypothalamus. The hypothalamus affects energy intake by regulating how much is eaten and how much energy is expended. Damage to the hypothalamus disrupts the balance between energy intake and expenditure, leading to increased caloric intake and/or decreased calorie burning, resulting in rapid weight gain, which can be difficult to reverse with currently available treatments (NORD, 2022).
Inflammation and Infection
Obesity influences the immune response, which can lead to susceptibility to infections. Excess adipose tissue causes proinflammatory pathways to be activated and can lead to chronic low-grade inflammation. Macrophages play a key role as the main cellular component of the adipose tissue regulating the chronic inflammation and modulating the secretion and differentiation of various pro- and anti-inflammatory cytokines.
Weight gain typically causes hormonal and metabolic changes that lead to an increase in C-reactive protein levels in the blood, which play a role in the body’s innate immune system and is used as a biomarker of inflammation. The resulting inflammation impairs the body’s ability to process insulin, leading to higher glucose levels and liver fat accumulation, which further impairs insulin processing.
Inflammation also appears to play a major role in the development of obesity, increasing the risk for metabolic disease, atherosclerosis, various malignant tumors, and a host of immune-mediated disorders that are due to a chronic, systemic, inflammatory response (Brezinski, 2024; Savulescu-Fiedler et al., 2024).
Chronic Stress
Studies show links between chronic stress and obesity. Stress can cause weight gain by:
- Interfering with cognitive processes such as self-regulation
- Increasing levels of hormones and chemicals involved in hunger, such as leptin and ghrelin
- Causing overindulgence in foods that are high in calories, fat, and sugar
- Disrupting sleep
- Depleting energy levels and causing people to engage in less physical activity
When stress is experienced, the body reacts by releasing the stress hormone cortisol, which triggers the fight-or-flight response. This slows down the digestive processes by diverting blood flow away from the digestive tract and toward the muscles and organs essential for immediate survival. Chronic exposure to cortisol leads to enlarged intestines, resulting in more nutrient absorption and obesity.
High levels of cortisol also interfere with the way the body produces other hormones, including corticotropin-releasing hormone (CRH). This hormone helps control appetite, so low levels may lead to higher food intake (Mayo Clinic, 2023b; Weber, 2023).
Gut Microbiota
Gut microbiota is a collection of trillions of microorganisms that live within the gastrointestinal tract. These microorganisms include over a thousand species of bacteria as well as viruses, fungi, and parasites. The microbiota produces both short-chain fatty acids that feed the cells in the gut lining and the enzymes needed to synthesize certain vitamins, including B1, B9, B12, and K.
There is overwhelming evidence that the composition of the gut microbiota and its metabolites impact the progression of obesity and obesity-related diseases. Gut microbiota provides crucial signaling metabolites, substances made or used when the body breaks down food, drugs or chemicals, or its own tissues including fat or muscle. This process produces energy and the materials required for growth, reproduction, and maintaining health. It also helps rid the body of toxic substances.
The composition and characteristics of the gut microbiota, as well as the factors affecting their homeostasis, are different between stages of infancy and between infants and adults. Gut microbiota disruption is associated with aging, antibiotic exposure, underlying diseases, infections, hormonal variations, circadian rhythm, and malnutrition, either alone or in combination.
Importantly, gut microbiota metabolites—including those that are biochemically modified by gut bacteria and produced by the host, but also those that are produced by bacteria from dietary components—play a vital important role in the development of obesity and related diseases (Geng et al., 2022; Cleveland Clinic, 2023).
Prenatal Factors
Intrauterine environment can shape the trajectory of weight gain and body fatness throughout the course of life. Three prenatal factors are the mother’s smoking habits, weight gain, and blood glucose levels during pregnancy.
MATERNAL PRENATAL SMOKING
Smoking during pregnancy is associated with increased child overweight independent of maternal prepregnancy weight as well as maternally transmitted and nontransmitted genetic predisposition to adiposity. Avoidance of smoking during pregnancy may help prevent childhood obesity irrespective of the mother–child genetic predisposition (CDC, 2023b; Schnurr et al., 2022).
MATERNAL WEIGHT
The offspring of pregnant women with obesity are at increased risk of developing obesity in childhood and as adults. Having one parent with obesity increases the risk of obesity by two- to threefold; two parents with obesity increases the risk up to 15-fold.
In utero nutritional excess and development in an obesogenic environment may lead to permanent changes of fetal metabolic pathways, raising the risk of childhood and adult diseases, such as hypertension, hyperglycemia and insulin resistance, hyperlipidemia, coronary artery disease, obesity-increased adiposity, and metabolic dysfunction-associated steatotic liver disease (Ramsey & Schenken, 2024).
MATERNAL BLOOD SUGAR LEVELS
High blood sugar during pregnancy increases an infant’s risk of being born too large and developing obesity or type 2 diabetes in the future (CDC, 2024b).
Gestational diabetes (GDM) starts when the body is not able to use the insulin it needs during pregnancy, leading to hyperglycemia. Gestational diabetes causes the pancreas to produce more insulin, but it is not able to lower blood glucose levels. The insulin does not cross the placenta to the baby, but glucose and other nutrients do. This gives the infant high blood glucose levels, causing the baby’s pancreas to make extra insulin to process the blood glucose. Since the infant is getting more energy from the extra blood glucose than it needs, the extra energy is stored as fat. In addition, children exposed to gestational diabetes have stronger brain responses to food cues, particularly in reward-processing regions, increasing risk of overeating and obesity (Zhao et al., 2024).
Postnatal Factors
The postnatal environment is just as significant to setting the pace of weight gain throughout life. Modifiable postnatal factors that affect weight in later life include:
- Rate of infant weight gain. Children with accelerated infant growth have an increased risk for being overweight. Children with fast fetal growth and subsequent accelerated infant growth have the greatest risk of being overweight at 5–9 years (Leth-Møller et al., 2024).
- Breastfeeding initiation and duration. A meta-analysis of 17 studies reported that a longer duration of breastfeeding is associated with a lower risk of weight gain in infancy, with each month of breastfeeding reducing the risk by 4% (Masood & Moorthy, 2023). Among infants born in 2019, most (83.2%) started out receiving some breast milk. At 1 month of age, 78.6% were receiving some breast milk. At 6 months, 55.8% of infants received some breast milk, and 24.9% received breast milk exclusively (CDC, 2024c).
- Infant sleep duration. Sleep regulates glucose metabolism and neuroendocrine function. Lack of sleep reduces glucose intolerance, insulin sensitivity, and leptin levels and increases the levels of cortisol and ghrelin (and, therefore, appetite). It has been found that infants who slept fewer than 12 hours a day had double the odds of being overweight by the age of 3 years, compared with infants who slept more than 12 hours a day. If a 3-year-old sleeps less than 10 and a half hours each night, there’s almost double the chance of obesity by age 7. Factors associated with shorter sleep duration included maternal depression during pregnancy, early introduction of solid foods (before 4 months), and infant television viewing (Masood & Moorthy, 2023; DiLonardo, 2024).
Ultraprocessed Foods
Ultraprocessed foods are industrial formulations made mostly or completely from substances (oil, fat, sugar, starch, and protein) extracted from food or derived from hydrogenated fats or modified starches then reassembled to create shelf-stable, tasty, and convenient meals. They can also be synthesized in laboratories with flavor enhancers, colors, and additives to make them highly palatable. These foods typically have five or usually many more ingredients. Ultraprocessed foods currently make up nearly 60% of what the typical adult eats and nearly 70% of what children eat.
Ultraprocessed foods tend to be low in fiber and high in calories, salt, added sugar, and fat. High consumption of these foods has been linked to health concerns, including increased risk of obesity, hypertension, breast and colorectal cancer, and premature death from all causes. Research, however, has not completely identified exactly what it is about this category of food that appears to cause these issues.
A 2019 study was done to compare the ultraprocessed diet to one based on minimally processed foods featuring fruits, vegetables, and unprocessed meats. Participants were served twice as many calories as needed to maintain their body weight and told to eat as much or as little as they wanted. Both diets were nutritionally matched, containing the same total amount of fat, sugar, salt, fiber, carbohydrates, and protein. When eating the ultraprocessed diet as compared to eating the unprocessed diet, participants were found to consume about 500 calories per day more and gained more weight and body fat, putting on an average of two pounds (Valicente et al., 2023; Godoy, 2023).
ULTRAPROCESSED FOODS AND GUT MICROBIOME
Diet has a pivotal role in shaping the composition, function, and diversity of the gut microbiome, with various diets having a profound impact on the microbial community within the gut. Studies have suggested that food processing promotes changes in foods such as inclusion of acellular nutrients, additives, and novel chemicals, which can then impact gut microbiota that promote an inflammatory microbiome.
In addition to differences in gut microbiota, higher ultraprocessed food consumption has been found to be positively related to leptin levels, which is related to leptin resistance. Leptin signals the body that there are sufficient energy stores, reducing hunger. Leptin resistance is associated with proinflammatory conditions, neuroinflammation, and metabolic disorders (Ross et al., 2024).
ADDICTIVE POTENTIAL OF ULTRAPROCESSED FOODS
Preclinical and human studies have demonstrated that repeated intake of ultraprocessed foods triggers addictionlike biologic (e.g., dopaminergic sensitization) and behavioral (e.g., withdrawal, continued use despite consequences) responses, whereas consumption of naturally occurring foods has demonstrated limited or no associations with addiction indicators.
This differentiation has been attributed to ultraprocessed foods sharing pharmacokinetic properties with addictive substances, namely those containing artificially high doses of rewarding ingredients (e.g., added sugars) that are rapidly absorbed by the system. Researchers recently argued that ultraprocessed foods meet the same scientific criteria used to define tobacco products as addictive.
Both addictive drugs and ultraprocessed foods can induce cravings in the same reward area of the brain, as demonstrated by functional magnetic resonance imaging (fMRI). Reward signals from highly palatable foods may override signals of fullness and satisfaction. Compulsive overeating is a type of behavioral addiction that triggers intense pleasure. Those with food addiction lose control in regard to overeating behavior and spend excessive amounts of time involved with food and overeating or anticipating the emotional effects of compulsive overeating (Zaraska, 2023; Goodman, 2023).
SALT
Throughout evolutionary history, salt has been a vital necessity for survival, and it has been a very rare resource. As a consequence, humans have evolved neuronal pathways for a habitual salt craving, which cannot be controlled. The importance of salt to overall health may explain why salty foods are so tasty and “you can’t eat just one.” Sodium appetite is an important instinctive behavior with high survival value, as there are many physiologic and cellular functions that depend on salt.
Neuronal mechanisms help drive the lust for salt. Neurons in the central amygdala become highly active when salt is being consumed. This area of the brain controls many innate and conditioned behaviors, including appetite-related and feeding behaviors. When we consume salt, the central amygdala is activated and dopamine is released, which triggers the brain’s reward system. This process is part of our evolutionary heritage to ensure our ancestors sought out this essential mineral (Research Features, 2023).
INDUSTRIAL SEED OILS
Industrial seed oils are derived from nuts, legumes, oilseeds, or fruits. They’re made by a chemical process in which these items are bleached, refined, and heated. Seed oils are a type of vegetable oil that come from the seeds of crops and contain high levels of linoleic acid, an e-omega-6 polyunsaturated fatty acid. Linoleic acid is needed by the human body in small amounts, but the excessive quantities found in seed oils can contribute to chronic diseases such as obesity, cardiovascular disease, and diabetes.
Seed oils that have moderate to high amounts of linoleic acid include:
- Soybean oil
- Canola oil
- Rapeseed oil
- Corn oil
- Sunflower oil
- Safflower oil
- Grapeseed oil
- Rice bran oil
Oils that are extracted from fruits have low to moderate amounts of linoleic acid:
- Olive oil
- Avocado oil
- Coconut oil
- Palm oil
(H & S Crew, 2024)
When oils (fats) are detected in the upper intestine, the message is carried up the vagus nerve through the hindbrain to the striatum. Foods rich in fat can increase dopamine in the striatum as much as 160% to 200% above normal levels, similar to what is observed with nicotine and alcohol, which produce feelings of pleasure and reward (Yang, 2024).
GLUCOSE AND FRUCTOSE
Excessive sugar consumption is linked to obesity primarily because it contributes to increased calorie intake, often with little nutritional value, and can lead to a build-up of fat in the body. Additionally, sugary drinks and foods can disrupt appetite-control signals and promote weight gain by not providing the same feeling of fullness as solid foods.
There are two main types of dietary sugars, glucose and fructose, with fructose being sweeter than glucose. (Sucrose, or table sugar, is a combination of fructose and glucose.) Both have an identical molecular formula but different structural formulas. Glucose consists of an aldehyde group, while fructose consists of a ketone functional group.
Both glucose and fructose are harmful when consumed in excess. What makes fructose more harmful is the way in which the body metabolizes it. Unlike glucose, which is used by cells as an energy source, fructose is metabolized by the liver, where it promotes synthesis of fat. Some of the fat can lodge in the liver, contributing to fatty liver disease. High fructose consumption is also linked to insulin resistance, metabolic syndrome, type 2 diabetes, and obesity.
In the past, fructose was a rare treat found in honey or seasonal fruit. Today, high fructose corn syrup (HFCS), which is made from cornstarch and contains approximately 55% fructose, is found in most processed foods and sugary drinks (Leech, 2023).
Growing evidence indicates that daily fructose consumption leads to some pathological conditions, including memory impairment. Fructose intake induces neuroinflammation, mitochondrial dysfunction, and oxidative stress. Subsequently, these mechanisms can trigger long-term effects, such as inhibition of neurogenesis, downregulation of trophic factors and receptors, weakening of synaptic plasticity, and long-term potentiation decay. In addition, it significantly affects several functions regulated by the nervous system, such as the sleep–wake cycle, locomotor activity, feeding behavior and energy homeostasis, as well as cognitive impairment (Franco-Pérez, 2024).
NOVA CLASSIFICATION SYSTEM
The NOVA classification system, developed by researchers at the University of Sao Paulo, Brazil, places all foods into four groups:
- Group 1: Unprocessed or minimally processed foods
- Meat, poultry, fish, and seafood
- Eggs
- Milk
- Fresh, frozen, or dried fruit
- Leafy and root vegetables
- Grains (brown or white rice)
- Legumes (beans, lentils, chickpeas)
- Group 2: Processed culinary ingredients
- Salt (mined or from seawater)
- Sugar (cane or beat)
- Butter and lard (milk and pork)
- Starches from corn and other plants
- Vegetable oil (crushed from olives or seeds)
- Group 3: Processed foods
- Canned or bottled vegetables, fruits, and legumes
- Salted or sugared nuts and seeds
- Salted, cured, or smoked meats
- Fruits in syrup
- Cheeses and unpackaged freshly made breads
- Group 4: Ultraprocessed food and drink products
- Sodas and sweetened drinks, including energy drinks
- Sweet or savory packaged snacks
- Confectionery and industrialized desserts (e.g., ice cream)
- Mass-produced packaged breads and buns
- Cookies, pastries, cakes, and cake mixes
- Margarine and other spreads
- Sweetened breakfast cereal
- Sweetened and flavored yogurts
- Preprepared meat, cheese, pasta, and pizza dishes
- Packaged meatballs
- Poultry and fish nuggets and other reconstituted meat products
- Meat products that contain preservatives other than salt
- Frozen or shelf-stable instant meals
- Instant noodles and instant or canned soups
- Baby formula and other baby food products
- Weight-loss products such as meal replacement shakes and powders
(MacMillan, 2024)
Medications
Weight gain as a result of certain prescription medications is known as iatrogenic obesity. Many commonly used medications list weight gain as a frequent side effect. Research has found that patients taking certain prescription medications gained weight, ranging from a few pounds to 10% or more of their body weight.
Each class of medication may trigger weight gain through different mechanisms. Some stimulate appetite. Others affect metabolic rate, which can result in weight gain despite not changing dietary habits. Some medications influence how the body stores and absorbs sugar and other nutrients.
Weight gain from prescription medications also increases the risk of a multitude of other complications, including metabolic syndrome, type 2 diabetes, and cardiovascular disease.
Medications that can result in weight gain include:
- Antidepressants
- Amitriptyline
- Citalopram
- Sertraline
- Nortriptyline
- Paroxetine
- Anticonvulsants
- Pregabalin
- Gabapentin
- Carbamazepine
- Valproic acid
- Antidiabetics
- Glipizide
- Insulins
- Glyburide
- Pioglitazone
- Antipsychotics
- Olanzapine
- Quetiapine
- Clozapine
- Perphenazine
- Antihypertensives
- Atenolol
- Metoprolol
- Propranolol
- Antihistamine and steroids
- Diphenhydramine
- Prednisone
(Dietz, 2023b)
Insufficient Physical Activity
Physical activity refers to any body movement that burns calories, whether for play or work. Exercise, a subcategory of physical activity, refers to planned, structured, and repetitive activities with the goal of improving physical fitness and health.
Most weight loss occurs from decreasing calories, but the only way to maintain weight loss is to engage in regular physical activity. Regular physical activity is a vital necessity for good health. Physical activity helps to reduce blood pressure and reduce risks for type 2 diabetes, osteoporosis, heart attack, stroke, certain cancers, as well as obesity. It can relieve symptoms of depression and anxiety, improve sleep, reduce risk of falling, improve cognitive function in older adults, and maintain a healthy weight.
Despite this recognition of the need for an increase in physical activity, however, recent statistics show that:
- Only 1 in 3 children are physically active every day.
- Less than 5% of adults participate in 30 minutes of physical activity each day, and only 1 in 3 adults receives the recommended amount of physical activity each week.
- Only 35%–44% of adults ages 75 years or older are physically active, and only 28%–34% of adults ages 65–74 are physically active.
- 28% of Americans, or 80.2 million people, ages 6 and older are physically inactive.
- More than 80% of adults do not meet the guidelines for both aerobic and muscle-strengthening activities, and more than 80% of adolescents do not do enough aerobic physical activity to meet the guidelines for youth.
- Nationwide, 25.6% of persons with a disability reported being physically inactive during a usual week, compared to 12.8% of those without disability.
- Children now spend more than seven and a half hours a day in front of a screen (e.g., TV, video games, computer).
- Nearly one third of high school students play video or computer games for three or more hours on an average school day.
- Only six states (Illinois, Hawaii, Massachusetts, Mississippi, New York, and Vermont) require physical education in every grade, K–12.
- Only about 1 in 5 homes have parks within a half mile, and about the same number have a fitness or recreation center within that distance.
(Delta College, 2024)
Obesogenic Environment
The term obesogenic environment describes the sum of all influences on the development of obesity from living conditions and surroundings, including opportunities available in a society or institution that are shaped by its social organization and structure. Obesogenic environments particularly promote physical inactivity and unhealthy eating behaviors (Cunningham, 2024).
BUILT ENVIRONMENT
Neighborhood characteristics play a powerful role in shaping people’s health, and research has demonstrated the particular importance of built environment factors associated with human-made spaces that individuals engage with on a regular basis. This includes physical characteristics such as walkability, presence of sidewalks, walking paths, bike paths, green spaces, and recreational and sports infrastructures that promote physical activity and healthful behaviors, as well as factors like public transportation and zoning regulations that constrain individuals’ food environments (Nguyen et al., 2024).
“SCREEN TIME”
Screens are ubiquitous in today’s environment, and almost everyone’s daily routine includes them, including children. Most American children spend about three hours a day watching television. Despite what is claimed, videos that are aimed at very young children do not improve their development.
Added together, all types of screen time can total five to seven hours each day. Too much screen time increases risk for obesity because:
- Sitting and watching a screen is time that is not spent being physically active.
- TV commercials and other screen ads can lead to unhealthy food choices. Food ads aimed at kids are for products that are high in sugar, salt, or fats.
- Children eat more when they are watching TV, especially if they see ads for food.
Current screen-time guidelines include:
- Children under 2 should have no screen time.
- Limit screen time to 1–2 hours a day for children ages 2 and over.
More than two hours of daily screen time is also associated with decreased executive function, decreased inhibition, increased impulsivity and inattention, cognitive changes, binge eating, and loss of eating behavior control (Bleistein, 2022; NIH, 2023a).
FOOD AND NUTRITION ENVIRONMENT
What people choose to eat plays a large role in determining risk of overweight or obesity. People’s choices are shaped by the world in which they live. In the United States, physical and social surroundings influence what one eats and can make it difficult to choose healthy over unhealthy foods. The food and nutrition environment includes all the factors involved in the ability to access foods: the availability of foods, culture and ethnicity, parenting, marketing, and other significant factors.
Food Availability and Access
In 2023 in the United States, 47.5 million people lived in food-insecure households, including 7.2 million children (USDA, 2025). Food availability and access are predominantly influenced by the local environments, including surrounding neighborhood infrastructure, accessibility, and affordability barriers. Access to grocery stores that carry healthy food options is not distributed equitably across residential and regional areas.
Areas lacking access to affordable healthy foods are called food deserts and are found in:
- Suburban neighborhoods that lack grocery stores that offer health food options
- Rural areas and neighborhoods where the nearest grocery stores are too far away to be convenient or accessible
- Neighborhoods that are comprised of a majority of racial or ethnic minorities
- Areas, rural or urban, with a higher percentage of residents experiencing poverty
Urban, suburban, and rural areas can also be overwhelmed with stores that sell unhealthy calorie-dense and inexpensive “junk” foods, including soda, snacks, and other high-sugar foods. This is known as a food swamp. Presence of food swamps is a predictor of obesity, particularly in communities where people have limited access to their own or public transportation and experience the greatest income inequality.
Obesity rates are higher in schools that have nearby access to a greater number of fast-food restaurants and lower in schools with access to small grocery stores and upgraded convenience stores participating in initiatives to improve healthful offers. Schools that offer unhealthier items experience a faster increase in obesity rates over time.
Community-level efforts that have successfully improved children’s food environments include more available healthier reimbursable meals and a la carte options available in schools and convenience stores participating in community initiatives shown to carry healthier foods (Ohri-Vachasapti et al., 2023).
Transportation to grocery stores with affordable prices is critical to food-insecure households. It is challenging to use a combination of public transit and walking to go grocery shopping for several reasons. First, grocery bags can be heavy and hard to carry on buses, transfer may be required, and wait times can be long depending on when shopping is done. In addition, the built environment around grocery stores is often not pedestrian friendly.
Food affordability is another element in choosing where one can shop (Wainer et al., 2023).
Race/Culture/Ethnicity and Diet
In the United States, more than 1 in 5 children have overweight or obesity. Black and Latino children are disproportionately affected, with both having higher prevalence and incidence rates of overweight and obesity than their White counterparts. Systemic inequalities, such as racial discrimination and unequal access to education and healthcare, can perpetuate the cycle of poverty and food insecurity within marginalized ethnic groups. These structural barriers create additional challenges for individuals and families in accessing nutritious food.
Culture affects the circumstances in which we eat, the types of food we eat, whom we eat with, the times of the day that we eat, and the quantities we eat. Food is culture and presents an everyday actualization of one’s ethnic identity. Food contains childhood memories, religious meaning, and connections to one’s origins.
One key aspect of the connection between ethnicity and food insecurity lies in the cultural and dietary practices of different ethnic groups. Cultural traditions, beliefs, and preferences often shape the types of foods consumed within a community. These practices can influence food access and affordability, as traditional or culturally significant foods may be more expensive or less readily available in certain area.
Immigrant communities may face challenges in accessing the ingredients necessary for their traditional dishes, leading to a sense of food insecurity. Additionally, dietary restrictions or preferences based on religious or cultural beliefs can further exacerbate the issue. These factors can limit the options available to individuals and contribute to disparities in food security across different ethnic groups.
Socioeconomic factors play an important role in understanding the connections between ethnicity and food insecurity. Research has consistently shown that certain ethnic groups are more likely to experience poverty and lower income levels, which directly impact their ability to afford an adequate diet. Economic disparities, such as wage gaps and limited job opportunities, can contribute to higher rates of food insecurity among specific ethnic communities (Easy Sociology, 2024).
Family Mealtimes and Parental Feeding Styles
Studies have found that the influence of family mealtimes is correlated with improved dietary intake and healthier weight status. Family meals may contribute to the development of healthy eating habits within the family and may act as a powerful preventative factor in reducing child obesity rates. In the context of family meals, parents provide an important social referencing role and example for their children to learn healthy and appropriate mealtime behaviors that could help them lower their risk for obesity across their development into adolescence and adulthood (Jones et al., 2023).
Parental feeding practices are goal-oriented food-specific behaviors or actions carried out by parents either intentionally or unintentionally that affect their child’s attitudes, behaviors, or beliefs toward food.
Parental feeding style affects children’s eating behaviors. Feeding styles are determined by a combination of demandingness and responsiveness. Demandingness refers to the degree to which a parent encourages a child to eat, while responsiveness refers to the way in which the parent encourages the child to eat, whether in a responsive or non-responsive manner. Parental feeding styles reflect the overall attitude and emotional climate characterizing eating occasions and reflect differences in parental demandingness and responsiveness. Feeding styles include:
- Authoritative feeding style is characterized by high demand and high response and is defined as reasonable nutritional demands in conjunction with sensitivity toward the child. This style is generally considered to be the best approach to prevent childhood obesity, as it has been associated with lower intake of snack foods and better dietary quality in meals.
Three negative feeding styles have been found to be linked to overweight and obesity. These include:
- Authoritarian (as opposed to authoritative) style uses strict rules, high standards, and punishment to regulate a child’s behavior. Authoritarian style involves coercive control and shows low responsiveness to the child’s wishes. It involves low support for child autonomy in eating and shows little trust in a child’s hunger/satiety signs. Example: A child cleans her plate even though she is full in order to please her parents. Effect: Ignoring a child’s appetite may lead to loss of ability to regulate internal hunger and fullness cues.
- Permissive/indulgent style involves making few demands, having very few rules and low expectations, using discipline sparingly, catering to the child’s food preferences, and providing a low level of control. This style is often linked with high intake of sweets and high-fat foods. Example: A child has eaten a cookie for dessert and demands more. The parent’s response is, “Okay, you can have as many as you want.” Rewarding is another example of an indulgent style. Example: A parent tells a child at the dinner table, “If you eat all your broccoli, I’ll take you out for ice cream.” Effect: The child tends to become out of touch with what and how much to eat.
- Uninvolved/neglectful style includes low demands and low responsiveness to the child, lack of support, and lack of structure and control. Parents show low sensitivity to their child’s needs and fail to plan and prepare food in a regular, reliable manner, considering food and feeding to be a low priority. This style is not always a conscious choice but can be forced by circumstances, such as single parenting and working late shifts. Example: A child is hungry, but there is no response from the parent to provide a regular meal. Because they consider food and feeding to be a low priority, they have not gone shopping, and therefore no one prepares a meal. Effect: The child becomes preoccupied with food, worried, and anxious, causing over- or undereating (Nelson, 2023).
WORK ENVIRONMENT AND OCCUPATION
The type, hours, and place of work have been recognized as sources of adverse environmental exposures that can lead to overweight and obesity.
- The number of hours spent at work. Research studies show that working long hours on the job is associated with higher body weight, and this is magnified when people work in occupations that are primarily sedentary. For workers in sedentary jobs, every 10 additional work hours was found to be associated with an average weight gain of three to four pounds for men and two pounds for women (Leach et al., 2023).
- Rotating shift work has been identified as a risk factor for overweight or obesity. Working rotating shifts disrupts the body’s natural circadian rhythm, disrupting the body’s internal clock which regulates metabolism and appetite. When disturbed it can lead to hormonal imbalances that may increase risk of weight gain and obesity (Physicians Premiere, 2023).
- Night shift work is associated with a significant increase in waist circumference. Dyslipidemia is significantly associated with night shift workers, which is the result of disruption in the circadian rhythm. Raised proinflammatory markers in night shift workers increases the risk of metabolic syndrome (Ellis, 2023; Bahinipati et al., 2022).
- Blue-collar workers (which may include machine operators, construction workers, public safety workers, and sales/office workers) have a higher risk of obesity. Many of these workers believe that a physically active occupation provides sufficient physical activity for health. In addition, surveys of foods available in work environments have shown that many of the workers in these professions have little access to healthy foods while at work and little access to intervention that would support attempts to change behaviors. Worksite wellness features, such as onsite workout facilities or weight control programs, are lacking in worksites with a high proportion of blue-collar occupations (Crane et al., 2022).
- Work-related stress can exacerbate anxiety and negatively affect diet quality. Studies have shown that work stress is a crucial risk factor for the development of metabolic syndrome, which includes weight gain. Stress-induced hormonal imbalances can lead to dysregulation in carbohydrate metabolism, making further weight gain easier and weight loss more difficult. In addition, behavioral factors, such as comfort food eating or drinking, may exacerbate the effects of work stress on weight (Nuesana, 2024).
FOOD MARKETING
Advertisements for unhealthy foods are everywhere, and marketing to young people to “hook” them on food manufacturers’ products presents a very profitable investment. Food marketing takes advantage of the developmental vulnerabilities of children and adolescents. Adolescent brains are biased toward rewards, and they are more likely to respond to cues in the environment, such as marketing.
Studies from many countries have shown that television marketing of unhealthy foods frequently targets children. Internationally, unhealthy food advertisements are more frequent during children’s typical viewing times, during school holidays, on children’s channels, and around children’s programming.
A wide range of creative advertising strategies are used that are likely to appeal to young people. These include celebrity endorsements, animations, and promotional characters. International studies of television and other media have shown that these creative strategies were more common in the marketing of food to children than to adults.
Product packaging that includes the presence of cartoon characters has been found to influence taste perceptions in young children. In one U.S. study of children ages 4 to 6 years, the children believed a product with a cartoon character tasted better than the same food in a package without the character. In another U.S. study, children ages 3 to 5 years tasted identical pairs of food and drink but felt they tasted better if they were in McDonald’s-branded packaging.
Results from a study on brain activity found that food commercials produced larger brain responses than nonfood commercials in different areas of the brain, including the middle occipital gyrus, which has been shown to consistently respond to drug-related cues compared with nondrug cues. Among children, the right middle occipital gyrus had higher activation in response to food advertising exposure.
The whole occipital lobe plays a role in visual processing of food cues. The fusiform gyrus, which is part of the brain’s visual object recognition system, was found to be one of the main brain regions activated in response to viewing food pictures, as was the posterior cingulate gyrus (OEH, 2023; Arrona-Cardoza et al., 2023).
SLEEP DEPRIVATION
Sleep deprivation influences food selection and eating behaviors, which are mainly managed by the food reward system. Sleep-deprived individuals mostly crave palatable energy-dense foods. Consumption of meals may not change, but energy intake from snacks that are high in sugar and saturated fat are desired, leading to overweight and obesity.
This is due to an imbalance in the hormones ghrelin and leptin that regulate appetite. Leptin makes one feel full, and ghrelin makes one feel hungry. Leptin levels typically rise during sleep, so if a person is not getting adequate sleep, the leptin levels decrease and hunger increases, which can lead to excessive foot intake and weight gain. Likewise, sleep disruptions of any kind can cause an increase in ghrelin, resulting in hunger (Wojeck, 2023).
Sleep deprivation also affects weight by having an impact on physical activity and energy expenditure. Sleep allows muscle tissue time to recover between workouts. Sufficient sleep is also important in having the energy to exercise. Lack of adequate sleep can lead to being less physically active during the day and reduced muscle strength. Sleep deprivation can also affect the safety of exercise, with increased sports injuries reported by those who are sleep deprived (Newsom & Rehman, 2024).
The human body generally runs on a sleep–wake cycle that lasts a little over 24 hours. This is known as the circadian rhythm. These rhythms are mostly the result of exposure to light and darkness, and they affect sleep, body temperature, hormone production, appetite, and other body functions. Insufficient sleep and circadian disruption are important metabolic stressors and are associated with weight gain and obesity. Circadian rhythm disruptions can result from:
- Brain damage or disruption in brain activity
- Damage to the eyes, retinas, or optic nerves
- Jet lag (traveling east advances the sleep cycle and tends to cause more severe jet lag than traveling west, which delays the sleep cycle)
- Working overnight shifts
Historically, eating would occur during daylight hours and sleep during night time hours. Today, this may not always be true. Irregularity in meals, such as eating at inconsistent times, skipping meals, and changing the frequency and number of meals, all influence the circadian clock and metabolism (Johns Hopkins, 2025a; NIH, 2023b; Cleveland Clinic, 2024).
COMORBITIES AND CONSEQUENCES OF OBESITY
Overweight and obesity boost the risk of death by anywhere from 22% to 91%, which is significantly more than previously believed. It is estimated that about 1 in 6 deaths are related to excess weight or obesity (Marshall, 2023).
In Adults
DISEASES AND HEALTH CONDITIONS
Obesity is a systemic issue that affects multiple organ systems and may lead to many diseases and health conditions (see table below).
| Body system | Diseases/conditions |
|---|---|
| (Lim & Boster, 2024; Hamdy, 2025; Perreault & Laferrère, 2024) | |
| Cardiovascular |
|
| Respiratory |
|
| Endocrine |
|
| Central nervous system |
|
| Musculoskeletal |
|
| Gastrointestinal |
|
| Urinary tract |
|
| Reproductive |
|
| Psychiatric/psychological |
|
| Integumentary |
|
| Infections |
|
| Neoplasms |
|
COGNITIVE EFFECTS
Neuroimaging studies have shown structural and functional changes in the brains of individuals with obesity (Saeed et al., 2025).
Obesity is associated with chronic low-grade inflammation throughout the body, including in the brain. This systemic neuroinflammation can dysregulate the hypothalamic–pituitary–adrenal (HPA) axis, impacting cortisol rhythms and potentially contributing to mood disorders and cognitive impairments. This obesity-induced disruption coupled with changes in cortisol secretion is thought to affect brain structures such as the hippocampus, further influencing cognitive function and potentially increasing the risk of neurodegenerative diseases.
Over time, brain cell damage may be secondarily due to an increase in the release of inflammatory cytokines by the adipose tissue that impairs cognitive function. Obesity has also been linked to vascular changes that promote atherosclerosis, and reduced blood flow to the brain can lead to cognitive decline and neurodegenerative changes. Obesity-induced systemic inflammation and metabolic dysregulation contribute to blood–brain barrier (BB) disruption, leading to various neurological disorders (Feng et al., 2024).
Alterations in gut microbiome composition and function may also play a role in the influence of obesity on executive functions. Excess adipose tissue contributes to a proinflammatory state that promotes growth of pathogenic bacteria over beneficial ones. This dysregulation of the gut microbiota can lead to increased intestinal permeability and further systemic inflammation (Allied Digestive Health, 2024; Wright et al., 2024).
MUSCULOSKELETAL EFFECTS
Overweight and obesity places added force and stress on the body’s joints, especially in high-impact areas such as the knees, hips, and ankles. Research shows that for every one pound of weight gained, there is an additional four pounds of force exerted on the knee joint. Over time this excess strain accelerates breakdown of protective cartilage drastically increasing the risk for developing pain and debilitating conditions like osteoarthritis.
Obesity makes bones more susceptible to cracking or breaking. Carrying extra weight also impacts bone health, increasing the risk for fractures, especially in the spine, wrists, and ankles (CORE Institute, 2024).
In Children and Adolescents
Obesity affects children and adolescents across all age groups, and the increasing prevalence of childhood and adolescent obesity is associated with a rise in comorbidities previously considered “adult diseases.” In the United States, close to one third of children over age 2 are overweight or have obesity, and for the first time since the 1900s, life expectancy for children is eroding because of obesity (Martinelli, 2022).
DISEASES AND HEALTH CONDITIONS
Obesity in childhood and adolescence can lead to severe health conditions, including:
Endocrine
- Prediabetes (increases the risk for developing type 2 diabetes mellitus)
- Type 2 diabetes (leads to more rapid progression of diabetes-related complications in later life)
- Metabolic syndrome (a cluster of risk factors for type 2 diabetes and atherosclerosis, which includes abdominal obesity, hyperglycemia, dyslipidemia, and hypertension)
- Hyperandrogenism in females and risk for early-onset polycystic ovary syndrome characterized by hirsutism, menstrual irregularities, acne, acanthosis nigricans, and seborrhea; accelerated linear growth and bone age associated with marked hyperinsulinemia
- Gynecomastia in males related to the stimulating effects of fat on estrogen production
- Central precocious puberty, particularly in girls; earlier attainment of pubertal milestones, menstrual disturbances, polycystic ovary syndrome
- Alteration in thyroid status
- Nonalcoholic fatty liver disease related to ectopic fat aggregation
Cardiovascular
- Essential hypertension, best assessed using ambulatory blood pressure (BP) monitoring rather than casual office BP measurement
- Dyslipidemia, particularly in those with central fat distribution and increased adiposity, including elevated concentrations of LDL cholesterol and triglycerides and decreased concentration of HDL cholesterol
- Alterations in cardiac structure and function similar to those seen in middle-aged adults, including increased left ventricular mass, increased left ventricular and left atrial diameter, greater epicardial fat, and systolic and diastolic dysfunction
- Cardiac fibrosis and impaired systolic and diastolic function related to abnormal lipid metabolism, including excessive activity of adipocyte cell signaling molecules, as well as oxidative stress and inflammation, which can potentially cause cardiac fibrosis and impaired systolic and diastolic function
- Premature atherosclerotic cardiovascular disease with endothelial dysfunction of the blood vessels, aortic intima-media thickening, development of early aortic and coronary arterial fatty streaks and fibrous plaques, and increased arterial stiffness
Gastrointestinal
- Nonalcoholic fatty liver disease, the most common cause of liver disease in children, resulting in fatty infiltration and inflammation of the liver
- Cholelithiasis (gallstones), with obesity being the most common cause in children (greater for girls than boys) without predisposing conditions, the risk increasing with increasing BMI
- Gastroesophageal reflex disorder and a higher risk of esophageal adenocarcinoma
Pulmonary
- Obstructive sleep apnea (complete obstruction of the upper airway during sleep and cessation of air movement despite ongoing respiratory effort)
- Alveolar hypoventilation syndrome (Pickwickian syndrome) during wakefulness, a rare but life-threatening disorder that requires prompt diagnosis and therapy
- Hypoventilation during sleep in the absence of airway obstruction, possibly due to the restrictive ventilator defect caused by abdominal distribution of fat
- Increased predisposition for respiratory infections and bronchial asthma
- Adverse effects on lung and chest mechanics, as well as a reduction in lung compliance
Orthopedic
- Slipped capital femoral epiphysis, typically occurring in early adolescence, related to increased shear forces at the capital femoral growth plate
- Idiopathic genu valgum (commonly called knock-knees), characterized by deviation of the knees toward the midline of the body
- Tibia varus (Blount disease), characterized by progressive bowing of the legs and tibial torsion as a result of excessive abnormal weight bearing, more commonly among individuals with darkly pigmented skin
- Fractures, since bone development is not always able to compensate for excess weight, with the resulting imbalance putting undue stress on developing bones
- Increased risk for joint damage or osteoarthritis in adulthood
- Pain, injuries, and fractures due to obesity-induced biomechanical change in gait pattern and greater joint burdens
- Impaired postural control
- Diminished bone mineral density
Neurologic
- Idiopathic intracranial hypertension (pseudotumor cerebri), in which increased intracranial pressure is observed with the absence of a mass, which presents with signs and symptoms of a brain tumor and can result in severe visual impairment or blindness
- Migraine incidence and progression
- Psychosocial
- Depressive conditions
- Eating disorders
- Attention-deficit/hyperactivity disorder (ADHD) and low self-esteem
- Anxiety, self-harm, and suicidal tendencies
Dermatologic
- Intertrigo, an inflammatory rash caused by skin-to-skin friction in warm, moist areas of the body
- Furunculosis (boils) or small abscesses involving hair follicles
- Hidradenitis suppurative, or inflammatory nodules or deep fluctuant cysts in the skin of the axillae and groin
- Acanthosis nigricans, or areas of dark velvety discoloration in body folds and creases, particularly the armpits, groin, and neck, associated with insulin resistance
- Striae distensae (stretch marks) caused by mechanical factors, possibly acting in concert with hormonal factors such as high levels of adrenocorticosteroids
(Skelton & Klish, 2024a; Ciezju et al., 2024; Balasundaram & Krishna, 2023)
COGNITIVE EFFECTS IN CHILDHOOD AND ADOLESCENCE
Overweight and obesity in childhood and adolescence are risk factors not only for general health but also for proper brain development and cognitive functions. Research has found a link between childhood obesity and alterations in brain structure, especially in the prefrontal cortex, affecting decision-making, response inhibition, working memory, and cognitive flexibility (Vandoni et al., 2024).
Metabolic alterations induce a peripheral systemic inflammatory process that can affect the blood–brain barrier and the functioning of brain regions linked to learning and memory processes. Obesity affects the functioning of the hippocampus and produces a decrease in the prefrontal cortex gray matter, thereby modifying cognitive abilities, especially executive functions (Marti-Nicolovius, 2022).
MOTOR EFFECTS IN CHILDHOOD AND ADOLESCENCE
Body composition in children and adolescents is related to the normal development of performance and gross motor coordination, and obesity can affect these. Strength, bilateral and upper limb coordination, running speed, balance, and agility are just some examples of motor activities that develop in early childhood.
Increased fat mass accumulation has been associated with a higher probability of developing a coordination deficit. Obesity results in poor performance in fine-motor precision and in manual dexterity, which can be due to difficulties with the integration and processing of sensory information.
Children with obesity show worse performance in locomotor skills due to biomechanical limitations, including:
- An increase in compressive and shear forces on the capital femoral growth plate that can alter the femoral angle
- A decrease in hip and knee flexion, resulting in stiffness while walking
Increased fat mass accumulation has been associated with a higher probability of developing coordination deficits. Children with obesity often have difficulties with coordination, including:
- Clumsiness
- Problems with gross motor coordination (jumping, hopping, balancing on one foot)
- Problems with visual or fine-motor coordination (e.g., writing, tying shoelaces)
(Vandoni et al., 2024)
PSYCHOLOGICAL/PSYCHOSOCIAL EFFECTS IN CHILDHOOD AND ADOLESCENCE
Psychological effects refer to an individual’s thoughts, emotions, and behaviors; psychosocial effects refer to the interactions and relationships between an individual, family, peers, and community.
Children and adolescents with obesity experience increased risk of social isolation and poorer peer relationships, discrimination, harassment, and self-esteem. Evidence suggests that obesity is also linked to lower social and physical indicators of quality of life, as well as deteriorated dimension of parent- and school-related psychological well-being.
Research has shown that psychopathology is more frequent in children with obesity when compared to adolescents without obesity. Mental disorders such as anxiety, eating disorders, depression, and attention-deficit/hyperactivity disorder (ADHD) often accompany obesity.
Those with obesity are more likely to report suicidal thoughts and attempts and are at greater risk for receiving a psychiatric diagnosis. Being male or with extreme obesity are most strongly associated with mental health comorbidity (Galler et al., 2024).
Children with obesity who have comorbid health problems such as diabetes, asthma, or sleep apnea miss school more frequently, negatively affecting their school performance.
Research has shown that individuals with obesity are more likely to not complete their education, due to adverse experiences (weight bias) within the school setting, which refers to marginalization by peers and teachers. More particularly, these experiences seem to be more frequent for girls compared to boys.
Among adolescents and young adults who were tracked after seven years, females who are overweight were found to have completed less schooling, were less likely to have married, and had higher rates of household poverty compared with their peers who are not overweight. For males who are overweight, the only adverse outcome was decreased likelihood of being married (Kokka et al., 2023; Schwarz, 2023).
Effects of Weight Bias and Stigma
Research suggests that weight bias and stigmatization have been increasing in the last decades. Prejudice and discrimination against individuals with obesity are ubiquitous within U.S. culture; even young children have been found to regard their peers who have obesity in negative ways. The bidirectional nature of weight stigma suggests that not only is a higher weight associated with higher likelihood of experiencing weight stigma, but weight stigma is associated with increasing weight.
Stigmatization is mostly based on a misunderstanding of the complex causes of obesity, with people attributing weight gain to personal responsibility, resulting in blaming people with obesity for their condition and enabling the negative stereotyping of them to flourish.
Healthcare providers have been identified as one of the most frequent perpetrators of weight stigmatization. Weight stigma in the healthcare setting threatens the therapeutic relationship between healthcare providers and their patients and families.
WEIGHT STIGMA AMONG YOUTH
In early school years, children with overweight and obesity may become targets of discrimination by their peers. Prejudice and stigmatization toward peers with overweight have been found as early as 3 years of age. A study done of male school children found that obesity was associated with peer stereotyping of negative characteristics, which included laziness, lying, cheating, ugliness, dirtiness, and stupidity. In another study, schoolchildren preferred children with a variety of disabilities to children with obesity to be their friends. Despite these issues, there are many young children with overweight and obesity who appear to maintain a positive self-image and have normal self-esteem.
Adolescents with obesity also experience bias and bullying from their peers. Many, particularly females, develop a negative self-image that persists into adulthood (Skelton & Klish, 2024b; Baile et al., 2022).
Weight bias in educational settings can come from a variety of different sources. Students are not just victimized by their peers. It has been documented that even their teachers (particularly, but not exclusively physical education teachers) can be common perpetrators of stigma.
Weight stigma can prevent students from progressing into higher education. Students with obesity are significantly less likely to be accepted to a college or university, and those who are admitted are likely to receive less financial support than their peers without obesity (World Obesity, 2022).
WEIGHT STIGMA IN THE WORKPLACE
Weight discrimination in the workplace persists. In most states, employees can be fired because of their weight. Currently, there are no federal laws protecting an individual from weight-based workplace discrimination. Michigan is the only state that has passed a law explicitly prohibiting weight-based discrimination, and the Washington State Supreme Court has declared that obesity is covered under their antidiscrimination law. Several other states are considering legislation to make weight-based discrimination illegal, including Massachusetts, New Jersey, New York, and Vermont. Several large cities have also prohibited workplace weight discrimination, including San Francisco and Washington, DC.
Stigma is present at every point in the employment process. This includes career counseling, interviewing and hiring practices, salary disparities, fewer promotions, harsher disciplinary actions, and higher termination rates. Workers with obesity are less likely to work in a sales or customer-facing position and are paid less than their peers without obesity for the same work. This is more pronounced for women than men, who can receive up to 6% less pay for the same work. Men with obesity may tend to sort themselves into lower-paying jobs (World Obesity, 2022; Dietz, 2024).
WEIGHT STIGMA IN CLOSE RELATIONSHIPS
Close relationships, including spouses/partners, children, parents, and siblings, have been found and documented to be the most common source of stigmatizing comments. In some cases, this source of stigma generates the most harmful stigmatizing encounters.
Parents of children with obesity may experience weight stigma by association, which may have direct repercussions for them, their children, and the parent–child relationship (World Obesity, 2022; Lee et al., 2022).
WEIGHT STIGMA IN THE MEDIA
Weight prejudice is apparent in almost all forms of media, including children’s shows, in which characters with obesity are often stereotyped as clumsy, lazy, and without friends, through to news reports that have apportioned blame for global warming and rising fuel prices to people with obesity. In terms of representation, characters who are underweight are significantly over-represented and characters who are overweight are under-represented compared to the general population, particularly in women.
Marketing for weight-loss product regimes is overwhelmingly focused on personal responsibility for weight, further perpetuating the belief that weight gain or loss is entirely in the hands of the individual. Overly discriminatory language is a predominant aspect of the obesity media narrative and will often be accompanied by equally stigmatizing images perpetuating the many false stereotypes attributed to people with obesity (World Obesity, 2022).
PROMOTING BODY POSITIVITY
Body positivity is a movement that emphasizes acceptance of one’s physical appearance and celebrating what the body can do rather than how it looks.
PRINCIPLES OF BODY POSITIVITY
- Acceptance: recognizing and valuing bodies of all shapes, sizes, and appearances without judgment
- Self-love: cultivating a loving and forgiving relationship with oneself; celebrating one's body and its capabilities
- Inclusivity: acknowledging and respecting the diversity of human bodies, including those of different races, genders, abilities, ages, and sizes
- Health at Every Size (HAES): promoting health and wellness without focusing on weight loss as a primary objective
- Rejecting diet culture: challenging the idea that weight loss is necessary for health or desirability
- Holistic well-being: recognizing that true wellness comes from nurturing the mind, body, and spirit rather than adhering to societal beauty standards
- Empowerment: encouraging individuals to feel confident in their own skin and make choices that are right for their bodies
- Support and compassion: fostering a supportive community that uplifts everyone in their body positivity journeys
- Critical media literacy: developing a critical understanding of how media and advertising impact body image and working to change the narrative around beauty standards
- Celebration of diversity: valuing and promoting the visibility of all body types in media, fashion, and beyond
(Lily, 2024)
Promoting a positive body image is generally a good thing. Research has shown that body image is closely linked to mental health and weight management. However, critics argue that the body positivity movement ignores the health risks associated with carrying excess body weight. For instance, obesity raises the risk of developing diabetes, high blood pressure, joint problems, breathing problems, and gall bladder disease (West, 2022).
As a result, many are now moving toward what’s called body neutrality, which is the idea that people can exist without having to think too much about their bodies one way or the other, de-emphasizing the focus on appearance. Body neutrality is associated with a more positive body image and better mental well-being (Swami, 2022).
WEIGHT STIGMA IN HEALTHCARE SETTINGS
Weight bias and stigma exists in healthcare settings. Healthcare providers often view obesity as an avoidable risk factor that impedes their ability to treat and prevent disease. Weight stigma in healthcare outcomes can include:
- Fewer preventive health services and exams
- Less access to cancer screening tests, such as pelvic exams and mammograms
- More frequent cancellation or delay of appointments
- Less time spent with the healthcare provider
- Less intervention and less discussion with the healthcare provider
- Avoiding seeking healthcare
Healthcare personnel have all shown a propensity to ascribe stereotypical characteristics such as being lazy, weak-willed, and noncompliant to patients with obesity. Physicians generally have lower levels of respect for patients with obesity and generally spend less time providing consultations to them compared to other patients. Physicians can also be a direct source of stigmatizing comments. In one study, 53% of people with overweight and obesity reported having received inappropriate comments from their doctor about their weight (Puhl, 2023).
Nurses may also view individuals with obesity as noncompliant, overindulgent, lazy, and unsuccessful. Studies of self-reported attitudes among nurses indicate that:
- 31% “would prefer not to care for individuals affected by obesity”
- 24% agreed that individuals affected by obesity “repulsed them”
- 12% “would prefer not to touch individuals affected by obesity”
In addition to stigma arising from the clinician–patient relationship, many people with obesity report a stigmatizing physical healthcare environment, which can include gowns, blood pressure cuffs, chairs, and examination tables that are unable to accommodate people with obesity (OAC, 2025; Fulton & Srinivasan, 2023; World Obesity, 2022).
BULLYING AND WEIGHT
Weight-related negative stereotypes lead to weight stigmatization, which translates into bullying. Bullying is a serious and widespread problem with detrimental consequences for the physical and mental well-being of children. It is described as unwanted behavior from a person or group that is either:
- Offensive, intimidating, malicious, or insulting
- An abuse or misuse of power that undermines or humiliates
- Causes physical or emotional harm to someone
Teens with obesity are twice as likely to be bullied as their peers without obesity. With regard to gender, boys with obesity experience an increased risk of bullying behaviors compared to girls with obesity (Cheng et al., 2022).
CASE
At the Longview Bariatric Center, in order for the bariatric team to better understand the issues of stigma and discrimination, a group counseling session was offered to participants willing to talk about their experiences of being overweight. The session was scheduled to last 90 minutes and was headed by Bria, a bariatric nurse practitioner. Seven individuals were enrolled, four women and three men between the ages of 23 and 42.
Following introductions, Bria explained the purpose of the session and asked the participants to describe some of their experiences of interactions socially, at work, in education, and in healthcare. Initially, people were reluctant to share these feelings because, as one participant, Sheila, said, “It’s so hard to talk about.”
Bria asked Sheila to explain, and she replied, “Well, I know people look at me and think, ‘She’s fat and ugly.’ It’s written on their faces—a look of pity or disgust. They don’t say it, but it’s obvious.” Another member of the group, Rick, added, “Sometimes they don’t even try to hide it.”
Everyone in the group described how their social interactions were impacted, with the strongest impact being on the younger women in the group. “People just don’t want to spend time to get to know you when you’re big,” said Latoya.
Among the group, many had experienced discrimination in looking for employment as well as in their workplaces. Helene reported that when she had applied for a job once, “they said they couldn’t employ me because I was too big to sit at their reception desk. I didn’t project the image they wanted for the company. I felt mortified.”
In the area of schooling, Latoya said, “I remember getting teased in school about my weight and coming home every day in tears. Sometimes the other kids would call me ‘rhinoceros’ or ‘tubby.’ I would hide in the bathroom at lunchtime so I didn’t have to go to the playground.”
When Bria asked the group about their experiences with healthcare professionals and in medical settings, it led to a vigorous discussion. The majority in the group said they didn’t like having their doctors bring up their weight because they didn’t have any useful advice and didn’t say anything they did not already know.
Sheila: “Oh, they say, ‘You just have a virus, and maybe you should lose some weight.’”
Rick: “Yeah, you go in because you’ve got a bad headache, and the doc says, ‘It’s because you’re overweight.’”
Latoya: “They think you’re stupid! They say, ‘You need to stop eating so much. You need to get out and be more active. You should do this … you should do that’ … stuff all of us already know. Get this! I went to my doctor a while back for a prescription for birth control pills, and he looked at me and said, ‘You mean you’re having sex?!’”
Logan: “Oh, yeah, people look at us like we’re some kind of asexual creature.”
Mason: “I was in the hospital two months ago for surgery on my foot. The hospital gowns were too small, and the bed was too small!”
As Bria listened, many of the participants expressed how they felt judged as being lazy and stupid. They expressed negative feelings about average-weight people, and Jenny said, “Don’t you just hate them!” Bria understood those statements to be an indication of the severity to which the participants felt victimized and judged by others.
At the end of the 90 minutes, Bria thanked them all for their willingness to talk about their experiences and offered to meet with them again should they wish to do so.
(Adapted from Hayden et al., 2010)
ASSESSING FOR OVERWEIGHT AND OBESITY
Nurse practitioners, office and clinic nurses, school nurses, hospital nurses, physical therapists, and occupational therapists, among others, all play a role in the assessment and treatment of children, adolescents, and adults for overweight or obesity. Assessment guidelines include:
- Body mass index or other screening or diagnostic tool measurement
- Classification of overweight and obesity
- Past medical history
- Health history, including
- Weight history
- Weight-loss efforts
- Physical activity
- Exercise habits
- Eating patterns
- Appetite control
- Family history
- Social history
- Review of systems
- Physical examination
- Diagnostic testing for comorbidities
(Mayo Clinic, 2023c)
Calculating Body Mass Index (BMI)
The primary way a person is categorized as overweight or obese is by calculating body mass index, which expresses the relationship (or ratio) of weight to height. BMI is calculated as:
(Weight in pounds ÷ height in inches2) × 703
or
Weight in kg ÷ height in meters2
BMI continues to be used as a screening tool because it is a quick, inexpensive, and reliable screening measure that is easier than other methods and does not require technical equipment and training. However, BMI can be misleading because it does not directly calculate body fat and is not, therefore, diagnostic (CDC, 2024d).
Certain factors that contribute to BMI inaccuracy include:
- Biological and genetic differences among racial and ethnic groups are not taken into account.
- Athletic individuals tend to have a higher percentage of lean muscle mass and lower percentage of fat mass, which might place them incorrectly in the overweight category.
- Two people can weigh the same and have the same BMI, but risk for disease might not be the same depending on how the weight is distributed. BMI does not include waist circumference.
- BMI in the high-normal to overweight range in older adults may be protective against developing certain diseases and dying early.
(Cleveland Clinic, 2022b)
BMI AND WEIGHT STATUS FOR ADULTS
BMI for adults 20 years and older is interpreted using standard weight status categories. These categories are the same for men and women of all body types and ages. The standard weight status categories are shown in the table below.
| BMI | Weight Status |
|---|---|
| CDC, 2024e | |
| <18.5 | Underweight |
| 18.5 to <25 | Healthy weight |
| 25 to <30 | Overweight |
| 30 to <35 | Class 1 obesity |
| 35 to <40 | Class 2 obesity |
| ≥40 | Class 3 obesity (severe) |
BMI AND WEIGHT STATUS FOR CHILDREN
BMI is interpreted differently for children and teens even though it is calculated in the same manner as adult BMI. The BMI in children and teens needs to be age- and sex-specific since the amount of body fat changes with age and differs between boys and girls. All children older than 2 years should have their BMI calculated at least annually from measured height and weight.
After BMI is calculated for children and teens, it is expressed as a percentile. The percentile can be obtained from either a graph or a percentile calculator, which expresses a child’s BMI relative to other children of the same age and sex. BMI-for-age percentile growth charts are the most commonly used indicator to measure the size and growth patterns of children and teens in the United States. A child BMI percentile indicates how a child’s measurements compare to other children of the same sex and age. For example, if a child has a BMI in the 75th percentile, 75% of children of the same sex and age have a lower BMI.
| BMI range | BMI category |
|---|---|
| *Ages 2 to 19 years. For children under age 2, consult WHO Child Growth Standards. (CDC, 2024f) |
|
| <5th percentile | Underweight |
| 5th to <85th percentile | Healthy weight |
| 85th to <95th percentile | Overweight |
| ≥95th percentile | Obesity |
| 120% of the 94th percentile or greater, or ≥35 kg/m2 | Severe obesity |
Other Screening and Diagnostic Tools
BMI has long been used as a way to define obesity in the United States, but experts are becoming increasingly critical of the approach, saying it does not paint a full picture of our health. Other tools are available, and the choice of the method for measuring weight or body fat composition depends on whether it is being obtained for clinical purposes or research and what degree of precision is required.
Other options that can be used to determine overweight or obesity include the following:
- Skinfold thickness uses calipers to determine how much body fat sits on top of muscle. It is a useful way of determining where the biggest fat deposits are.
- Dual energy X-ray absorptiometry (DXA body scan)estimates fat-free mass, body fat, and bone mineral density. It is generally the preferred method in a clinical setting when a more rigorous determination of body composition is needed. Two beams are used to scan the body. One beam is absorbed more by fat than the other, so the computer can differentiate fat from other tissues, providing a percentage of body fat. It uses a very low dose of radiation and is fairly simple for an operator to perform. It has been validated against other techniques and is widely considered the gold standard for measuring body tissue, bone, muscle, and fat.
- Waist circumference measures central adiposity, which is associated with an increased risk of morbidity and mortality. The National Heart, Lung, and Blood Institute (NHLBI) and American Heart Institute (AHI) define a healthy waist size as:
- ≤35 inches for women
- ≤40 inches for men
- The International Diabetes Federation defines a healthy waist size as:
- ≤31.5 inches for women (31.4 inches for Chinese, Japanese, and South Asian women)
- ≤35.5 for men (35.4 inches for Chinese, Japanese, and South Asian men)
- Waist-to-hip ratio (waist circumference divided by hip circumference) is a measure of fat distribution. Those with abdominal adiposity are at increased risk of comorbidities. Men with a waist–hip ratio of 0.95 or more and women with a ratio of 0.85 or more are considered to be at increased cardiovascular risk.
- Bioelectrical impedance analysis (BIA) is simple and widely used and relies on an electrical current to measure the fat and fat-free mass of the body. Accuracy in placement of electrodes is essential, as variations can result in large errors. Impedance is measured by applying electrodes to one arm and one leg or by having the individual stand on the foot plates of a special scale. BIA is less reliable than DXA body scan.
- CT or MRI imaging techniques can reliably determine patterns of body fat distribution. It is possible to obtain an accuracy of <1% margin of error using a series of scans.
- Nuclear magnetic resonance spectroscopy is similar in technology to MRI but is capable of discerning fat and glycogen within tissues as well as fat and lean mass overall.
- Hydrodensitometry (underwater weighing) is based on the fact that lean body tissue is denser than fat. It has been largely replaced by DXA.
- Whole-body plethysmography uses air displacement rather than water displacement. The person is placed sitting inside a special enclosed chamber after being weighed on a scale to determine mass measurement, and sensors determine the amount of air displaced by the person’s body. Body fat and lean muscle mass can then be calculated (Perreault, 2023; Phillips & Shulman, 2023).
- Relative fat mass index (RFM) is a newer, better measure of body fatness than many indices currently in use, including BMI. RFM calculates the amount of fat present in relation to an individual’s height and weight, providing a more accurate measurement of fatness than traditional methods. RFM has gained importance in recent years due to its ability to provide a more precise evaluation of body fat levels. Unlike BMI, which only considers weight and height, RFM considers the distribution of fat in the body, making it a more reliable indicator of overall health and risk of obesity-related diseases.
- RFM is obtained simply by measuring height and waist circumference and plugging the figures into the following formula:
- Men: 64 – (20 × height/waist circumference) = RFM
- Women: 76 – (20 × height/waist circumference) = RFM
(Calculator Academy Team, 2024)
| Interpretation | Fat Level, Men (%) | Fat Level, Women (%) |
|---|---|---|
| (Michalowska, 2024) | ||
| Extremely low | <2 | <10 |
| Essential fat | 2–5 | 10–13 |
| Athletes | 6–13 | 12–20 |
| Fitness | 14–17 | 21–24 |
| Average | 18–24 | 25–31 |
| Obese | 25+ | 32+ |
Past History
Determining a patient’s past history is focused on investigating the cause of obesity or overweight and should include:
- Onset of weight gain. Early onset of obesity with dysmorphic features may point toward genetic causes.
- Developmental delay and intellectual deficits, which may be indicative of genetic causes of obesity.
- Menstrual history. Irregularities can occur in polycystic ovarian syndrome (PCOS), Cushing’s syndrome, hypothyroidism, menopause, or even pregnancy.
- Presence of other medical conditions, including type 2 diabetes mellitus, fatty liver disease, osteoarthritis, cardiovascular disease, obstructive sleep apnea, heart failure, and cancer.
- History of cranial radiotherapy or surgery leading to hypothalamic disorders and obesity.
- Family history of excess weight and other medical conditions.
- Drug history, including medications that can cause weight gain, such as antidepressants, antipsychotics, insulin, anti-epileptics, corticosteroids, and even topical formulations.
- Social history, including alcohol intake, socioeconomic background, and ethnicity, which might make it more challenging to adopt a healthier lifestyle.
- Diet history, including speed of eating and eating environment. Eating disorders, mental health conditions and hypothalamic disorders can result in overeating. Autonomy in creating meals might not always be possible for all, such as for people in supported living settings.
- Allergies and intolerances.
- Physical activity and sleep. Insufficient sleep and circadian misalignment can contribute to weight gain. Modern working patterns and lifestyles, such as shift work and late-night screen time, result in sleep disruption and should be taken into consideration.
- History of weight-loss attempts and lifestyle and treatment modalities used.
(Mallik et al., 2023)
Review of Body Systems
An inventory of body systems is completed in order to identify signs or symptoms a person may be experiencing or has experienced related to overweight and obesity, including:
- Obesity secondary to genetic syndromes, hormonal disease, iatrogenic medications
- Polycystic ovary syndrome (oligomenorrhea or amenorrhea)
- Low testosterone level, low sex drive, or erectile dysfunction in men
- Obstructive sleep apnea, hypoventilation syndrome
- Osteoarthritis in adults
- Foot, hip, or knee pain (orthopedic issues, slipped capital femoral epiphysis in children)
- Urinary stress incontinence (related to body mass and pressure)
- Abdominal pain (gastroesophageal reflux disease, gallbladder disease, pancreatitis)
- Disability/immobility
- Blurred vision, history of glaucoma, diabetic retinopathy
- Psychological disorder or stigmatization, anxiety, depression, ADHD, PTSD, social isolation
- Medications being taken for depression or anxiety
- Polyuria, polydipsia, polyphagia (type 2 diabetes mellitus)
- Headaches (idiopathic intracranial hypertension, aka pseudotumor cerebri)
- Obesity secondary to genetic syndrome
(AACE, n.d.)
Physical Examination
Physical examination includes obtaining vital signs, height, weight, and BMI and a complete head-to-toe examination in order to rule out any medical conditions that can be the cause of obesity and to assess for comorbid conditions.
General
- Sex, race, body build
- Obvious dysmorphic or distinguishing features that may suggest a genetic syndrome
- State of development in relation to chronological age (especially important in childhood and adolescence regarding evidence of secondary sex characteristics)
- Functional mobility, posture, gait
- Hygiene
Vital Signs
- Blood pressure. Elevated blood pressure may be a sign of Cushing’s syndrome. Normal blood pressure in adults ranges from 110/75 to 130/85. Pediatric blood pressure levels are interpreted based on sex and age (see table below).
| Age (years) | Systolic | Diastolic |
|---|---|---|
| (Mersch, 2025) | ||
| 1–2 | 90–105 | 55–65 |
| 3–5 | 95–107 | 60–71 |
| 6–9 | 95–110 | 60–73 |
| 10–11 | 100–119 | 65–76 |
| 12–15 | 110–124 | 70–79 |
Head, Eyes, Ears, Nose, and Throat
- Microcephaly, a feature of Cohen syndrome (aka Pepper syndrome)
- Poor linear growth in children, which may be due to hypothyroidism, Cushing’s syndrome (high levels of cortisol), or Prader-Willi syndrome (a rare disorder present at birth)
- Papilledema, an optic disc swelling secondary to elevated intracranial pressure seen in patients with pseudotumor cerebri
- Nystagmus or visual complaints, which may be related to hypothalamic-pituitary lesion
- Clumps of pigment in the peripheral retina, which may indicate retinitis pigmentosa (Bardet-Biedl syndrome)
- Tonsillar enlargement secondary to sleep apnea
- Erosion of tooth enamel resulting from self-induced vomiting in those with an eating disorder
Skin and Hair
- Acanthosis nigricans, seen in those who have diabetes or prediabetes (children with acanthosis nigricans being at high risk of developing type 2 diabetes later in adulthood)
- Hirsutism and excessive acne, which may be related to polycystic ovary syndrome
- Skin tags, seen commonly with insulin resistance
- Purple striae on the abdomen, lower flank, breasts, hips, buttocks, shoulders, upper thighs, upper arms, and axillae, which are caused by rapid weight gain due to Cushing’s syndrome
Cardiac and Respiratory
- To exclude cardiomegaly and respiratory insufficiency
Abdomen
- Abdominal tenderness, which may be related to gallbladder disease, GERD, or nonalcoholic fatty liver disease
- Hepatomegaly and hepatic tenderness due to nonalcoholic fatty liver disease
Genitourinary
- Undescended testicles, small penis, or scrotal hypoplasia, which can occur in children with Prader-Willi syndrome
- Small testes, which may suggest Bardet-Biedl syndrome
- Delayed or absent puberty
- Precocious puberty
Extremities
- Limited hip range of motion, which could suggest a slipped capital femoral epiphysis
- Lower-leg bowing caused by Blount disease, in which the medial side of the tibia, immediately distal to the knee joint, fails to develop normally
- Pes planus (flat feet) and pronation of the feet, common in children with obesity
- Dorsal finger callouses, which may indicate self-induced vomiting
- Malformed or misshapen body parts (extra digit next to the fifth digit may present in Bardet-Biedl syndrome, small hands and feet in Prader-Willi syndrome)
- Evidence of osteoarthritis
(Burridge et al., 2022)
Laboratory Studies
ADULTS
Standard laboratory studies in the evaluation of an adult patient with obesity include:
- Fasting lipid panel. At minimum, fasting cholesterol, triglycerides, and high-density lipoprotein cholesterol (HDL-C) levels should be done. Increased low-density lipoprotein cholesterol (LDL-C) and normal or marginally increased total cholesterol are not uncommon among persons with obesity.
- Liver function study results are normal in most persons with obesity. However, elevated transaminase levels may indicate nonalcoholic steatohepatitis (NASH) or fatty infiltration of the liver.
- Thyroid function tests. Although hypothyroidism itself rarely causes more than mild obesity, these tests can rule out primary hypothyroidism. Screening with a serum thyrotropin level is recommended as adequate. Thyroid-stimulating hormone (TSH) levels are commonly elevated in persons with obesity.
- Glucose and insulin studies. All persons with obesity should be screened for diabetes and prediabetes, including a fasting glucose and hemoglobin A1C (HbA1C).
Other laboratory tests should be done as indicated by clinical findings and suspicions. For example, when Cushing’s syndrome or other hypercortisolemic states are suspected, a 24-hour urinary free-cortisol test should be included (Hamdy, 2025).
CHILDREN AND ADOLESCENTS
Laboratory evaluation for children with obesity is focused on identification of any genetic or hormonal disorder that may be a cause of obesity in a child. The following is the suggested routine screening:
- Fasting lipid panel, done once between the ages of 9–11 and again between ages 17–21 for detection of dyslipidemia
- Glucose and insulin studies, including serum hemoglobin A1C level as well as fasting and two-hour glucose and insulin levels for evaluation of glucose tolerance and insulin resistance
- Thyroid function tests
- Liver function studies to screen for nonalcoholic fatty liver disease
In addition to the above, the following studies are included based on history and physical examination:
- Serum leptin level (recognizing that a genetic mutation lowers leptin level leading to decreased satiety)
- Adrenal function tests (recognizing that cortisol levels are commonly elevated in patients with obesity) to assess possibility of Cushing’s syndrome
- Karyotype with florescence in situ hybridization (FISH) for Prader-Willi syndrome
- Growth hormone secretion and function tests
- Assessment of reproductive hormones, including prolactin
- Serum calcium, phosphorus, and parathyroid hormones to evaluate for suspected pseudohypoparathyroidism
- MRI of the brain, when clinically indicated, with focus on the hypothalamus and pituitary
(Schwarz, 2023; AACC, 2022)
CASE
Kevin, age 7, was screened for overweight and obesity at school. He and his parents were referred to the nurse practitioner for assessment because Kevin had a steadily increasing BMI over the past six months. At the initial appointment, height and weight were obtained, and BMI was calculated and added to his current chart. He is now in the 92nd percentile for weight, which classifies him as overweight.
In taking a family history, the nurse practitioner learned that Kevin’s mother, age 32, has always been overweight and is constantly dieting to maintain her weight. She is also taking medication for hypertension. Kevin’s father is 33 years old. His weight has been in the healthy range all his life and his blood pressure is also normal. Kevin’s maternal grandmother, age 57, is overweight and has type 2 diabetes. His maternal grandfather is 58 and of normal weight; he recently suffered a stroke. Both paternal grandparents are in their late 50s and are of normal weight. The grandfather suffers from angina pectoris, and the grandmother is in good health. The nurse discussed Kevin’s increased risk for obesity and comorbidities based on this history.
A review of systems reveals that Kevin enjoys school and has a number of friends he plays with both at school and after school. His mood is most often upbeat. He has no symptoms of diabetes and denies headache or breathing difficulties. He sleeps eight to 10 hours every night. Kevin denies any abdominal discomfort and reports he has regular bowel movements. He denies any foot, hip, or knee pain. Kevin has no allergies to medications and is currently on no medications.
On physical examination Kevin is a White, well-developed, overly nourished, smiling young boy with a small frame and normal musculature, round trunk, and protruding abdomen. There are no obvious dysmorphic features. He has a normal gait, erect posture, and shows good hygiene.
- Vital signs: within normal limits, BP 105/65
- HEENT (head, ears, eyes, nose, throat): face symmetrical with no abnormalities; eyes, PERRLA, no papilledema; no tonsillar enlargement; thyroid normal; lungs, normal breath sounds; teeth in good condition
- Skin: overall even color; no areas of hyperpigmentation, growths, or striae; normal hair distribution
- Heart: normal heart sounds, regular rhythm, no murmurs
- Lungs clear to A and P
- Abdomen: presence of excess adipose tissue, normal bowel sounds, no evidence of discomfort or tenderness to palpation, no hepatomegaly
- Genitalia: normal for age penis, both testes descended, no hernias
- Extremities: no edema, normal pulses, no deformities, no gait deviations observed
Because Kevin is in the 92nd percentile for BMI and has risk factors (maternal overweight and hypertension and family history of stroke, cardiovascular disease, and type 2 diabetes mellitus), a fasting lipid panel and glucose levels are obtained. Liver function studies are deferred at this time. Fasting blood glucose is 80 mg/dl, cholesterol 150 mg/dl, and LDL 100 mg/dl, all of which are in the normal range.
MANAGEMENT AND TREATMENT OF OBESITY IN ADULTS
Effective management, as with all chronic medical conditions, must be based on a partnership between a highly motivated patient and a team of health professionals, which may include a physician, psychologist, psychiatrist, advanced practice nurse, social worker, case manager, pharmacist, physical therapist, occupational therapist, dietitian, and other specialists, depending on the person’s comorbidities. Scientific evidence indicates that multidisciplinary programs reliably produce and sustain modest weight loss between 5% and 10% for the long term.
Management strategies include:
- Lifestyle interventions using diet and physical activity
- Behavioral therapy, including assessing readiness for change
- Pharmacotherapy
- Surgery
Lifestyle Intervention for Adults
Initially, management requires the recognition that medical advice to “just eat less and exercise more” is not effective for patients to succeed at losing weight and maintaining that weight loss. Most individuals who are overweight or have obesity have already tried self-help approaches well before medical intervention is considered.
The patient’s weight management history can be a starting point in determining the choice of a treatment plan, which should begin with comprehensive lifestyle management, including diet, physical activity, and behavior modification. This plan should include:
- Self-monitoring of caloric intake and physical activity
- Goal setting
- Stimulus control
- Nonfood rewards
- Relapse prevention
WEIGHT-LOSS GOALS
An individual’s body weight and body fat are steadfastly regulated, and this highlights the importance of setting realistic weight-loss goals. Recognizing this, together with the value of modest weight loss, has led to a shift in the medical management of obesity from a goal of massive weight loss to one of maintaining the lowest possible weight while still eliminating obesity-related comorbidities or reducing them to a minimum. Data previously suggested that approximately 10% of body weight loss in persons with obesity is associated with substantial health benefits. Newer guidelines indicate that clinically meaningful health improvements can be seen with weight loss in the range of 2% to 5%.
The weight-loss goal for each patient must be individualized; however, a reasonable goal in the setting of a medical treatment program is approximately 1 to 2 pounds per week. Factors that are considered in setting a weight-loss goal include the weight of other family members as well as the patient’s cultural, ethnic, and racial background. There is evidence that greater weight loss can be achieved with a culturally adapted weight-loss program than with a more general health program (Hamdy, 2025).
DIET
Reducing total energy intake should be the main component of any weight-loss intervention. Current findings indicate that many types of diet can be successful in losing weight. The best predictor of success is dietary adherence. Therefore, providers are advised to recommend diets to improve adherence according to patient preference. Diet composition is important, but the key factor in promoting weight loss is a negative energy balance.
“Conventional” diets are defined as those with energy requirements above 800 kcal/day. These diets fall into the following groups:
- Balanced low-calorie diets and low-calorie versions of healthy diets, such as the Mediterranean diet and Dietary Approaches to Stop Hypertension (DASH) diet
- Low-fat diets
- Low-carbohydrate and low glycemic index diets
- High-protein diets
- Very low-calorie diets
- Intermittent fasting
“Fad” diets involving unusual combinations of foods or eating sequences may be popular but are not sustainable in the long term. The hallmark of a fad diet is restriction or elimination of certain foods. Examples of fad diets include:
- Atkins diet
- Zone diet
- Keto diet
- Grapefruit diet
- Paleo diet
- Gluten-free diet
- Master Cleanse
- Whole20
- Special K diet
(Perreault & Delahanty, 2024; Migala, 2024)
Low-Calorie and Reduced-Portion Diets
Balanced, low-calorie diets and reduced-portion diets are those that dietitians and other weight-management professionals most commonly recommend and that underlie most of the popular, commercial weight-loss programs. Although these diets are useful for short-term weight loss, none of them alone is associated with reliable, sustained weight loss.
In these diets, a reasonable goal for caloric intake is set and meal plans are then devised to provide this total, divided among three or more meals throughout the day.
Low-calorie diets considered healthy include:
- Mediterranean diet:
- Vegetables: four or more servings per day (one portion should be raw vegetables)
- Fruits: three or more servings each day
- Grains: four or more servings each day, mostly whole grains
- Fats/oils/olive oil: four tablespoons or more each day (choose extra virgin olive oil)
- Dried beans/nuts/seeds: three or more servings dried beans/nuts/seeds
- Fish and seafood two to three times each week
- Herbs, garlic, onions, and spices instead of salt daily
- Yogurt/cheese/egg/poultry daily to weekly
- Alcohol/wine: one to two glasses per day for men, one glass per day for women
(Cleveland Clinic, 2024)
- Dietary Approaches to Stop Hypertension (DASH) diet:
- Six to eight servings of grain/day
- Four to five servings of fruit/day
- Four to five servings of vegetables/day
- Two to three servings of fat-free or low-fat dairy/day
- Six or fewer 1-ounce servings/day of lean meats, poultry, or fish; or one egg
- Four to five servings of nuts, seeds, and legumes per week
- Two to three servings fats and oils/day
- Less than five servings per week of sweets and added sugars
Potential complications of low-calorie diets include:
- Vitamin deficiency
- Starvation ketosis
- Electrolyte derangements
- Cholelithiasis
(Mayo Clinic, 2023d)
Reduced-portion diets may be based on regular, everyday foods; by participation in a structured weight-loss program; or by incorporating products such as meal-replacement shakes, prepackaged meals, bars, and frozen entrees. These have adequate amounts of major macronutrients based on the food pyramid from the USDA and recommended daily allowances (RDAs). Alcohol, sodas, most fruit juices, and highly concentrated sweets are calorie dense and nutrient deficient and are generally prohibited or reduced to a minimum (Hamdy, 2025).
Very low-calorie diets (VLCDs) result in rapid weight loss and may be a suitable option in the short term. Many VLCDs are commercially made formulas of 800 calories or fewer that replace all the food one usually eats. VLCDs may be used in a clinical context to improve health markers. However, due to their low energy content, largely risking the loss of skeletal muscle mass, and their restrictive nature, it is likely not an ideal option for long-term weight loss/maintenance.
VLCDs are generally safe when used under proper medical supervision. They are not recommended for pregnant or breastfeeding women and are not appropriate for children or teens except in specialized treatment programs. They may also not be used in people over age 50, depending on the potential need for medications due to chronic illnesses as well as other possible side effects.
Reported side effects VLCDs include:
- Fatigue
- Constipation
- Nausea
- Diarrhea
- Cholelithiasis
Adverse effects can include hair loss, skin thinning, hypothermia, cholelithiasis, ketosis, vitamin deficiency, electrolyte derangement, and emotional problems (Zelman, 2024a).
Diets with Different Macronutrient Compositions
Macronutrients refer to carbohydrates, fats, and proteins. Some diets emphasize manipulation of these macronutrients in order to promote weight loss. There is moderately certain evidence that, over six months, most macronutrient diets result in modest weight loss and substantial improvements in cardiovascular risk factors. At 12 months, the effects on weight reduction diminishes and blood pressure improvements largely disappear (Ge et al., 2020).
Low-Carbohydrate Diets
While all low-carbohydrate diets reduce the overall intake of carbohydrates, there is no clear consensus on what defines a low-carb diet. However, a daily limit of 20 to 57 grams of carbohydrates is typical with a low-carb diet.
Low-carbohydrate approaches to weight loss are based on the hypothesis that lowering insulin, a critical hormone that produces an anabolic, fat-storing state, improves cardiometabolic function and results in weight loss. Studies thus far have shown low-carb diets, and specifically ketogenic diets, to be superior to other dietary approaches in producing rapid weight loss for the first six to 12 months. A low-carbohydrate diet includes:
- Lean meats, such as sirloin, chicken breast, or pork
- Fish
- Eggs
- Nonstarchy vegetables (e.g., leafy green vegetables, cauliflower, and broccoli)
- Nuts and seeds, including nut butter
- Oils, such as olive, coconut, and rapeseed
- Some fruits, such as apples, blueberries, and strawberries
- Unsweetened dairy products, including plain whole milk and plain Greek yogurt
When there is a lower intake of carbohydrates, the intake of fat and protein generally increases to compensate for the reduction. It is believed that low-carb diets produce rapid weight loss compared to other diets because fats and protein increase satiety and produce less accompanying hypoglycemia, which reduces hunger and overall food intake (Fletcher, 2023; Oh et al., 2023).
Types of popular-named low-carbohydrate diets include:
- Atkins
- Modified Atkins
- Low-carb Paleo
- Whole30
- Low-carb Mediterranean
- Dukan
- South Beach
- Zero-carb
- The Zone
The ketogenic (keto) diet is a version of a low-carbohydrate and high-fat diet. A keto diet does not provide enough calories from sources of glucose and other forms of sugar and causes the body to burn fat to create energy. When fat is broken down, ketones are released by fat cells into the bloodstream. The increase in blood ketones lowers the normal acid–base balance in blood to make it more acidic, a state known as nutritional ketosis (which does not produce metabolic ketosis). Types of ketogenic diets include:
- Carnivore diet (zero carb diet)
- Paleo diet (centers on unprocessed, truly natural foods)
Side effects when stopping carbohydrate intake can include:
- Constipation due to low fiber intake
- Hypoglycemia
- Decreased serotonin levels and increased risk of anxiety and depression
- Decreased uric acid levels, leading to kidney stones or gout flare-ups
- Muscle cramps
- Halitosis (bad breath)
- Risk of “keto flu,” which may include headaches, fatigue, brain fog, irritability, lack of motivation
(Oh et al., 2023; Sloan, 2024)
Low-Fat Diets
Low-fat dietary guidelines recommend reducing the daily intake of fat to 30% or less calories and decreasing saturated fats by replacing them with polyunsaturated fats. A general rule is that a food that provides 100 calories and has 3 grams or less of fat is considered a low-fat food. Very low-fat diets provide less than 10% to 15% of calories from fat. Low-fat diets:
- Limit foods that contain industrial sources of trans fats, such as partially hydrogenated oils
- Reduce intake from solid fats, such as from meats or butter, and use plant oils to replace these solid fats where possible
- Replace protein foods that are higher in solid fats (e.g., red and processed meats) with choices that are lower in solid fats and calories or are sources of oils, such as:
- Seafood
- Legumes
- Nuts
- Seeds
- Plant oils
- Soy products
- Lean meats
- Poultry
- Eggs
(Perreault & Delahanty, 2024)
Adverse effects of a diet that provides insufficient amounts of fat include dry skin, hair loss, and a weakened immune system, as well as:
- Vitamin deficiencies. A very low intake of fat-soluble vitamins A, D, E, and K may impact vision, skin, the immune system, hormone synthesis, bone health, and the nervous and reproductive systems.
- Poor brain function. Dietary fat, especially the essential fatty acids, is important for brain health and development, and low levels of unsaturated fats may impact cognitive function and mood.
- Hormonal imbalance. Women who do not get enough fat in their diet and have a body fat composition below the optimum may observe disruptions to their menstrual cycle and may experience fertility issues.
(Williams, 2023)
Types of popular low-fat diets include:
- Ornish diet
- Therapeutic Lifestyle Changes (TLC) diet
- Engine2
(Cleveland Clinic, 2024; NIH, n.d.; Schweitzer, 2024)
High-Protein Diets
High-protein diets have been recommended for obesity treatment because they can help build lean muscle (which increases the number of calories burned throughout the day) and are more satiating and stimulate thermogenesis. High-protein diets may also improve weight maintenance. Like low-carbohydrate diets, high-protein diets can produce a state of ketosis. Some high-protein foods include:
- Legumes
- Dried beans (black, pinto, kidney)
- Salmon, cod, halibut
- Vegetables (dark leafy greens, peppers, mushrooms, broccoli, cauliflower)
- Lean cuts of red meat
- Poultry (chicken breasts and thighs)
- Eggs
- Low-fat milk, cheeses, and yogurt
- Peanut butter
- Soy milk/tofu
- Whole grains (quinoa, amaranth, barley)
- Berries (blueberries, strawberries, raspberries)
- Nuts and seeds (almonds, walnuts, chia seeds, hemp seeds)
(Frey, 2024)
Popular high-protein diets include:
- Protein Power diet
(Zelman, 2024b)
Intermittent Fasting
Intermittent fasting is an eating plan that cycles between periods of fasting and eating on a regular schedule. There are many different intermittent fasting schedules one can follow, such as eating only during an eight-hour period each day and fasting for the remainder or eating only one meal a day two days a week. For example, the “5:2 approach” involves eating regularly five days a week and limiting intake for the next two days to one 500–600 calorie meal.
After hours without food, the body exhausts its sugar stores and starts burning fat (metabolic switching). During times when the person is not eating, water and zero-calorie beverages are permitted.
It is recommended that individuals who are undertaking intermittent fasting for weight loss use the Mediterranean diet as a guide for the types of foods to be eaten (see above).
Research to date has found that intermittent fasting:
- Boosts working and verbal memory
- Improves blood pressure and resting heart rates
- Improves physical endurance
Intermittent fasting is not recommended for:
- Children and teens under age 18
- Women who are pregnant or breastfeeding
- People with type 1 diabetes who take insulin
- People with a history of eating disorders
(Johns Hopkins Medicine, 2025b)
PHYSICAL ACTIVITY
Exercise/physical activity is a proven modality for treating overweight and obesity. A minimum of 150–300 minutes of moderate physical activity per week or 75–150 minutes of vigorous physical activity per week is essential to prevent weight regain, increase weight loss, and improve fitness. However, for individuals who wish to lose weight, at least 200–300 minutes of moderate-to-vigorous physical activity each week is recommended to encourage long-term weight loss.
Aerobic exercise is a form of physical activity proven to be efficacious in managing obesity. Moderate- or high-intensity aerobics involving larger groups of muscles are recommended. Exercise, including strengthening (resistance) exercises, increases muscle mass. Because muscle tissue burns more calories at rest than does fat tissue, increasing muscle mass produces lasting increases in basal metabolic rate. Exercise that is interesting and enjoyable is more likely to be sustained. A combination of aerobic and resistance exercise is better than either alone (Harvard T.H. Chan, 2025; Levy & Nessen, 2023; CDC, 2023b).
Calorie restriction (CR) in older adults increases the risk of inducing muscle and bone loss, and this increases the risk of frailty and disability. Therefore, combining CR with exercise training is a well-established approach among this population, as it induces fat mass loss while minimizing muscle and bone mass loss compared to CR or exercise alone (Colleluori & Villareal, 2022; Niemiro et al., 2023).
For patients who track calories taken in and expended, the table below can provide information on approximately how many calories are burned in 60 minutes during various activities.
| Exercise | 125 lbs | 155 lbs | 185 lbs |
|---|---|---|---|
| (Nunez, 2024) | |||
| Running | 652 | 808 | 965 |
| Water polo | 566 | 703 | 839 |
| Bicycling | 480 | 596 | 710 |
| Calisthenics | 480 | 596 | 710 |
| Circuit training | 480 | 596 | 710 |
| Jump rope | 453 | 562 | 671 |
| Stationary bicycling | 420 | 520 | 622 |
| Rowing machine | 420 | 520 | 622 |
| Aerobic dance | 396 | 492 | 587 |
| Swimming (casual) | 396 | 492 | 587 |
| Jogging | 396 | 492 | 587 |
| Hiking | 340 | 421 | 503 |
ENCOURAGING PHYSICAL ACTIVITY
Communities around the country are making efforts to encourage walking, biking, and other forms of physical activity. For example:
- After city officials installed a new bike lane in New Orleans, the number of cyclists increased by 22%.
- People who used outdoor fitness equipment in Los Angeles parks exercised 46% more frequently than those who did not.
- In five states, walking and biking to school increased by 37% after sidewalks and crosswalks were improved.
- In Houston, the number of children walking or biking to school increased by 125% after schools began participating in a “walking school bus” program, which involves a group of children walking to school together with one or more adults.
(Physiopedia, 2025a)
THE ROLE OF PHYSICAL THERAPY
Appropriate, targeted physical activity is a potentially powerful tool, both for helping to reduce obesity and for improving clinical outcomes related to numerous comorbid conditions (e.g., metabolic disease, cardiovascular disease, inflammation). Physical therapists are an important part of the multidisciplinary team working with individuals with obesity. As specialists in body movement and functional mobility, physical therapists are able to use up-to-date evidence in order to design and teach individualized physical exercise/activity programs to help patients meet their unique weight loss and fitness goals.
Evaluation and treatment by a physical therapist can promote weight management and obesity prevention, address potential barriers to being active, minimize activity-related pain or discomfort, and identify which specific types and amounts of exercise are appropriate for an individual.
Physical Therapy Evaluation
The initial visit will include a full evaluation, including a detailed health history and questions about some or all of the following:
- Medical/surgical history
- Current level of physical activity
- Any activity-related difficulty or pain
- Medical conditions which may affect physical activity
- Current medications
- Patient’s individual functional mobility goals
The initial evaluation will also include examination of a patient’s strength, joint mobility, coordination, balance, and safety with performing physical mobility activities. Specific tests to further assess obesity—such as measurement of waist and skinfold thickness, body fat percentage, or BMI—may also be conducted. Consultation with patient’s physician or other members of the patient’s treatment team may take place as indicated in order to safely manage existing comorbid conditions, rule out any underlying medical needs, and otherwise coordinate care.
Physical Therapy Treatment
Using information gathered from initial evaluation, physical therapists create tailored activity programs, including both aerobic and strengthening exercises, to align with a person’s specific health goals, taking into consideration any existing conditions. Physical activities may be modified as needed to allow participation by individuals with orthopedic challenges, arthritis, chronic pain, physical disabilities, or other potentially limiting conditions. Some primary goals of a physical therapy activity plan for addressing obesity include:
- Pain reduction/minimization
- Improved cardiovascular fitness
- Improved muscle strength
- Optimized flexibility and posture
There is no one-size-fits-all approach to physical fitness, and each patient will require a program that meets their unique situation, needs, and goals. An effective physical therapy plan will also assist patients with identifying and overcoming barriers to regular physical activity, developing and maintaining healthy activity habits, and setting realistic personal goals (Avruskin, 2021; Physiopedia, 2025b).
Behavioral Modification
Changing behavior—especially long-term, habitual patterns—and getting oneself to do something different even when it is known to be the best thing to do, depends on an individual’s mindset. Mindset refers to the belief in one’s limitations. A fixed mindset focuses on what is known and the belief that basic abilities and talents are fixed traits that cannot be changed. A growth mindset focuses on improving what and how one does things. In order to lose weight and keep it off, people often must learn to think differently about what they eat, when they eat, and how they eat.
ASSESSING READINESS TO CHANGE
Efforts aimed at behavioral change begin with the clinician’s determination of a patient’s readiness to change as well as the readiness of parents and families of children and adolescents with obesity. One model for assessing such readiness is the Transtheoretical Model, which explores the individual’s feelings, awareness, judgments, perceptions, and behavior and describes the process of change using these five stages:
- Precontemplation. Individuals in this stage have no intention of changing or taking action within the near future, tend to defend their current habits, and become defensive in the face of other people’s efforts to pressure them to change. People are often uninformed about the consequences of overweight and obesity, they may have failed in the past to make changes or lose weight, or they may avoid seeking any information that would help change behavior.
- Contemplation. Although the person may think about the negative aspects of having obesity, they may doubt that the long-term benefits associated with change will outweigh the short-term costs. It may take as little as a couple of weeks or as long as a lifetime to move through the contemplation stage.
- Preparation (determination). In this stage, an individual begins researching and gathering information about what is needed to make a change and prepares a plan of action, such as a weight-loss or exercise program. At this stage they believe changing their behavior can lead to a healthier life. Individuals in this stage require assistance in the development and implementation of specific action plans and in setting realistic goals. Many times, people skip this stage and try to move directly from contemplation into action, which often results in failure.
- Action. This is the stage where people are motivated to make changes in behavior and lifestyle by using a variety of different techniques. This is the shortest of all the stages. The amount of time people spend in action varies and generally lasts about six months. Assisting a person can include providing problem-based learning experiences, support, and feedback.
- Maintenance. The person has made significant modification in behavior and lifestyle and has been successful in avoiding a return to prior behaviors. People in this stage tend to remind themselves of how much progress they have made, constantly reformulate the rules of their lives, and acquire new skills. They are able to anticipate situations in which they might return to old habits and behaviors and prepare coping strategies in advance. At this stage, it is important to continue to provide support, assist with problem-solving, positively address slips and relapses, and employ reminder systems or performance support tools.
(LLU, 2025)
INTERVENTION STRATEGIES
Interventions aimed at behavioral modification are considered essential in the management of the patient who is overweight or has obesity. Behavioral modification methods can be used either alone or in conjunction with other treatments, working to create goals, helping to maintain goals that have already been achieved, preventing possible relapses, and managing difficult situations.
Behavioral modification interventions include face-to-face contact and are often conducted in group sessions, which may be available at local hospitals, through commercial programs, or in office settings. While some patients might prefer individual therapy, the group setting may be more cost effective, and there is insufficient evidence to conclude that one is better than the other. All interventions use similar strategies, which include the following elements:
- Collaborative setting of realistic and achievable goals, which is meant to increase motivation and adherence. According to the “SMART” formulation, goals are specific, measurable, achievable, reasonable, and time-bound and should be within a patient’s control.
- Self-monitoring of food intake, weight, and activity, which is the most important step in successful behavior therapy. Self-monitoring slows down decision-making, allowing time to make healthier choices and alerting the individual about overconsumption and nutritional content of foods. Tools for self-monitoring can include keeping food diaries and activity records, internet applications, smartphone applications, and digital scales for self-weighing and recording.
- Stimulus control, which alters the person’s environment to help make better choices. Participants are educated in selecting fresh fruits and vegetables; preparing easy-to-eat, lower-calorie foods; placing them prominently in the refrigerator or on the counter; and removing less-healthy foods from the home. Stimulus control also includes setting the environment so the individual can concentrate on eating.
- Eating style, which involves slowing down the eating process to give time for physiologic signals for fullness to arise. Practicing “mindful eating” allows one to concentrate on tastes and textures of food and savor what is being eaten by chewing more slowly. Other techniques might involve leaving the table briefly during a meal and drinking water between bites or just prior to the meal.
- Portion control and meal planning, which provide a defined meal structure and can result in greater weight loss than the absence of such a structure. Use of portion-control plates or meal replacements are examples.
- Regular weighing as a self-monitoring strategy. This has been recommended in some studies. Concerns have been raised that regular weighing might lead to anxiety and weight regain, but this has not been observed in a systematic literature review.
- Increasing physical activity. Along with self-monitoring, increasing physical activity is a key element in successfully losing weight.
- Nutrition education and meal planning with a registered dietitian for assessment of knowledge and preferences.
- Social support enhancement to improve long-term weight loss. Behavioral programs that include strong family support provide both short- and long-term benefits.
- Other behavioral tools may include:
- Cognitive restructuring, such as changing self-talk (see below)
- Problem solving, such as managing food intake in difficult situations
- Assertiveness training, such as learning to say no
- Stress reduction, by identifying and reducing stressors that are triggers for eating
(Perreault & Burgermaster, 2024)
MOTIVATIONAL INTERVIEWING (MI)
While behavioral interventions provide a variety of strategies for change, motivational interviewing addresses the specific challenges of motivation, confidence, treatment readiness, ambivalence, and resistance. It is an approach that has also been shown to be successful for individuals with substance use disorders.
MI involves asking open-ended questions that encourage individuals to explore their thoughts, feelings, and motivations related to behavior change. MI assumes that behavior change is affected more by motivation than by information and that no lasting change will be achieved unless the patient sees the need to change. MI includes:
- Exploring ambivalence. Example: “What are some reasons you might want to make changes to your eating habits?”
- Eliciting importance and values. Example: “How does your weight impact your day-to-day life and your future goals.”
- Considering pros and cons. Example: “What are the positive aspects of losing weight, and are there any concerns or challenges you foresee in making these changes?”
- Exploring readiness for change. Example: “On a scale of 1 to 19, how confident are you about your ability to make changes to your eating habits?”
- Identifying goals. Example: “Where would you like to see yourself in terms of weight and health in the next few months?”
- Exploring confidence and self-efficacy. Example: “How do you think you could handle situations where you’re tempted to make unhealthy food choices?”
- Support systems and resources. Example: “Who in your life could provide encouragement and support, or what resources are available in the community that could assist you in your weight loss journey?”
(OMA, 2023a)
The core principles of MI are:
- Expressing empathy to create a safe space for exploration
- Supporting the person’s self-efficacy by emphasizing strengths and past successes
- “Rolling” with resistance by navigating around it
- Developing discrepancy by highlighting discrepancies between current behavior and goals or values
- Enhancing motivation by utilizing techniques such as reflective listening, open-ended questions, and affirmations
(Alomare, 2024)
CASE
Cynthia is a 15-year-old African American girl who is 5 feet, 3 inches tall and weighs 180 pounds, with a BMI of 31.9. She has been referred to the local health clinic by the school nurse at Winston Senior High School because of recent weight gain. The clinic’s nurse practitioner employs Motivational Interviewing to assist adolescent patients and their families in weight-loss efforts. During the first session with the family, the nurse found both parents to be very supportive and eager to help Cynthia meet the goals agreed on with the clinic’s weight-loss team.
Today is Cynthia and her parents’ second visit to the clinic, and the nurse practitioner utilizes MI in her meeting with the family.
Nurse: “Hello, Cynthia. Hello, Mr. and Mrs. Rockland. It’s good to see you all again. Tell me, how have things been going for you this past week?” (Asking an open-ended question)
Cynthia: “Oh, so, so. Mom and Dad have been after me to follow the plan, and I’m trying, but not very well, I’m afraid.” (Responding with elaboration)
Nurse: “You haven’t been completely successful sticking with the plan.” (Rephrasing)
Mom: “She’s trying, but not has hard as we think she could.”
Nurse: “You think she is not trying hard enough.” (Restating)
Mom: “Well …”
Cynthia (interrupting): “I really am trying hard, but there’s so many things that happen and get in the way!” (Emotional elaboration)
Nurse: “You sound a bit upset!” (Mirroring)
Cynthia: “I am! It’s really hard when you sit in the cafeteria and everyone else is eating the good stuff, and your lunch is a salad with a dinky piece of chicken in it!” (Elaboration)
Nurse: “It sounds like it’s hard to sit and watch others enjoying the foods you like but aren’t supposed to eat.” (Reflecting)
Dad: “I know just how she feels. I’ve been heavy all my life, and it’s very hard to give up those things you’ve always enjoyed.” (Empathizing)
Nurse: “I can certainly understand how you both feel.” (Empathizing)
Cynthia: “You know, it’s really hard. I didn’t gain any weight last summer but started gaining again when I went back to school this fall.” (Elaborating)
Nurse: “It sounds like you were successful in sticking to your diet last summer.” (Affirming)
Cynthia: “Yes, but when I went back to school, everyone around me was eating all the good things I like and can’t have.” (Elaborating)
Nurse: “You want to stick to your diet and lose weight, but you still want to enjoy the foods you like. That sounds like a dilemma to me.” (Summarizing)
Cynthia: “Yeah, that’s exactly it! But I really do want to be thinner like the other girls. I don’t want to be a fatty! I know I can do it, but sometimes it’s just so hard.” (Using “change talk”)
Nurse: “Well, let’s see. You say you want to be thin like the other girls, and at the same time, you’re saying that eating the foods you shouldn’t eat is very important to you.” (Developing and examining discrepancy)
Cynthia: “Yes, I don’t like to look the way I do, and I really want to try harder. I really do.” (Using change talk)
Nurse: “You really are strongly motivated to change and believe you can do it.” (Supporting self-efficacy)
Cynthia: “Yes, and I know Mom and Dad are really trying to help me.” (Using change talk)
Nurse: “I see. So, tell me what the three of you might do to make this wish happen.” (Finding out what the patient and family already knows)
Cynthia: “I don’t know what else I can do. I miss Taco Bell!”
Dad: “You and me both.”
Mom: “Well, I think I have a suggestion. Maybe we could all try to be more creative with the meals we make. Maybe we could explore some new recipes so your lunch is more exciting. We could start to cook together. How does that sound?” (Collaborating)
Dad: “That’s sounds like fun to me. When should we start?” (Encouraging)
Cynthia: “That does sound like fun. We’ve never cooked anything together before. Could we really do that?” (Collaborating and negotiating)
Nurse: “Would you be interested in meeting with the dietitian again to get some ideas about the foods you could make and some basic recipes?” (Asking permission, collaborating, negotiating a plan, empowering)
Cynthia: “Shall we do that, Mom and Dad? Yeah, let’s do that!” (Collaborative response)
Mom: “I would love to spend time with you in the kitchen.” (Agreeing on action plan)
Dad: “You know I like to cook, and Mom and I can share meal planning and cooking with you on alternate days of the week.” (Agreeing on action plan)
TECHNOLOGY AND BEHAVIORAL CHANGE
Devices such as wearable activity-tracking smartwatches and pedometers have been shown to be very useful tools for overcoming physical inactivity and obesity. Use of these devices is associated with increased physical activity, supportive behavior-change techniques such as self-monitoring and goal setting, improved BMI, and lower risk of developing obesity.
Pros:
- Gain sleep pattern insights
- Monitor cardiovascular health
- Motivation to stay active
- Personalized workouts and exercises
- Personal fitness goals
Cons:
- Apps may require a subscription
- Concerns around personal data privacy
- Cost
- Not 100% accurate (i.e., underestimate calories/steps)
(Beal, 2024)
THE ROLE OF OCCUPATIONAL THERAPY
Holistically minded occupational therapy practitioners have the skills to provide services to individuals, groups, and populations vulnerable to obesity. Occupational therapy practitioners are uniquely positioned to evaluate a person’s environmental and occupational factors to create a plan of care that is focused on establishing health-promoting routines and habits as well as modifying and optimizing a person’s environment to support appropriate weight management. Occupational therapy’s role in promoting health includes managing routines and habits around food consumption and patterns of occupation,
For example, the intervention Lifestyle Redesign, created by occupational therapists at the University of Southern California, focuses on strategies and opportunities to increase sustainable changes that lead to physical and psychosocial health. It promotes the identification of barriers and options to implement changes in the existing habits and routines using an interactive process of self-analysis and reflection about the relationship among occupation, health, and well-being in one’s everyday life. In Lifestyle Redesign, the therapist also evaluates the individual’s existing lifestyle patterns to create meaningful goals for lifestyle change that become the concentration of future occupational therapy (Muntefering et al., 2023).
Pharmacology
There are only a few drugs available for the treatment of obesity, and their effectiveness is limited to palliation rather than cure. Benefits fade when they are discontinued. All medications carry more risks than diet and physical activity interventions, and medications are used only in those patients for whom the benefit justifies the risk. They are not used during pregnancy or when breastfeeding.
Weight-loss drugs are considered for patients with a BMI >30 or a BMI >27 with a serious medical condition related to obesity (e.g., diabetes, hypertension) who have not met weight-loss goals (loss of at least 5% of total body weight at three to six months) with comprehensive lifestyle interventions.
Weight-loss drugs may not be effective for everyone. When used as part of a diet and exercise plan, typical weight loss is 5%–10% of body weight over a 12-month period.
Currently, there are three major categories of drugs used to manage obesity:
- Anorexiants are drugs that act on the brain to suppress appetite. They have a stimulant effect on the hypothalamic and limbic regions of the brain that control satiety.
- Stimulants are drugs that increase dopamine, which accelerates the autonomic nervous system and results in an increased energy expenditure.
- Lipase inhibitors impair the gastrointestinal absorption of ingested fat, which is then excreted in the stool.
(Hamdy, 2025)
| Drug | Category | Common side effects |
|---|---|---|
| * Ozempic is the same medication as Wegovy, but Ozempic is approved for type 2 diabetes and heart disease prevention; use of Ozempic for weight loss is considered off-label. (Perreault & Reid, 2024; Mayo Clinic, 2022; Anderson, 2025; Hamdy, 2025; NIDDK, 2024; Johnston, 2024) |
||
| Orlistat (Xenical), oral capsule | Lipase inhibitor | Allergic reactions, signs and symptoms of kidney stones or liver injury, uncontrolled or urgent bowel movements, black or bloody tarry stools |
| Phentermine-topiramate (Qsymia), oral capsule | Anorexiant | Dry mouth, constipation, numbness and tingling, dizziness, joint pain, insomnia, headache, nausea, taste changes, metabolic acidosis |
| Naltrexone-bupropion (Contrave), oral tablet | Anorexiant | Nausea or vomiting, dizziness, dry mouth, constipation, headache, seizures, mental disturbances such as suicidal thoughts, irritability |
| Liraglutide (Saxenda), daily injection | Anorexiant | Constipation, diarrhea, vomiting, nausea, abdominal pain and bloating, dizziness, fatigue, headaches, indigestion, gastroenteritis |
| Semaglutide (Wegovy*), weekly injection | Anorexiant | Nausea, diarrhea, vomiting, constipation, abdominal pain, headache, fatigue, dizziness, belching, low blood sugar in type 2 diabetes, flatulence, heartburn, runny nose, sore throat |
| Setmelanotide (Imcivree), weekly injection | Anorexiant/stimulant | Depression, darkened skin pigment, nausea, vomiting, stomach pain, headache, diarrhea, erection without sexual activity in males |
| Tirzepatide (Zepbound), weekly injection | Anorexiant | Nausea/vomiting, diarrhea/constipation, stomach pain or upset, indigestion, acid reflux, pain/itching/swelling/redness near injection site |
| Phendimetrazine (Bontril), extended-release capsule and tablet | Anorexiant/stimulant | Flushing, increased sweating or urination, dizziness, headache, blurred vision, dry mouth, nausea, diarrhea, constipation, stomach pain, irritability, increased or decreased interest in sex |
Researchers are studying several weight-loss pills in clinical trials, with notable supporting data so far for oral semaglutide, orforglipron, and amycretin. Other promising new weight-loss drugs that are currently being developed include:
- Injectable retatrutide
- CagriSema (cargrilintide and semaglutide)
- MariTive (maridebart cadfraglutide)
(Murdock, 2024)
Weight-Loss Surgical Procedures
Metabolic and bariatric surgical procedures are performed when diet and exercise have not worked or when the person has serious health problems due to weight. Some procedures limit much how can be eaten; others work by reducing the body’s ability to absorb fat and calories. Some procedures do both.
Bariatric surgery can offer many benefits; however, all forms of weight-loss surgery are major procedures that can pose risks and side effects. Individuals contemplating weight-loss surgery must be aware that they will need to make permanent healthy changes to their diet and perform regular exercise to help ensure long-term success.
Candidates for metabolic and bariatric surgeries (MBS) must meet at least one of the following criteria:
- MBS is recommended for individuals with BMI ≥35 kg/m2, regardless of presence, absence, or severity of comorbidities.
- MBS is recommended in patients with T2D and BMI ≥30 kg/m2.
- MBS should be considered in individuals with BMI of 30–34.9 kg/m2 who do not achieve substantial or durable weight loss or comorbidity improvement using nonsurgical methods.
It is recommended that surgery be performed by a board-certified surgeon with specialized experience/training in bariatric and metabolic surgery and at a center that has a multidisciplinary team of experts for follow-up care (ASMBS, 2024b).
The following conditions would disqualify a person from weight-loss surgery:
- Pregnancy
- Inability to commit to lifestyle changes necessary post surgery
- Cardiovascular, respiratory, or other medical conditions that make any type of surgery dangerous
- Autoimmune connective disease or a family history of one
- Presence of an infection
- Uncontrolled inflammatory disease of the gastrointestinal system
- Anatomical abnormalities of the esophagus, stomach, or intestines
- Certain bleeding disorders
- Past history of a gastric injury during a past surgery or through other circumstances
- Active cancer
- Untreated or uncontrolled mental health issue, attempted suicide in the recent past, or substance use disorder
A retrospective study analyzed patients over 65 years who underwent laparoscopic bariatric procedures and found bariatric surgery to be a safe and effective method of treatment of obesity in older adults (over 65 years of age). Patients over 65 years of age had improvement in T2D and hypertension after bariatric surgery (Dowgiatto-Gornowicz et al., 2023).
There are many benefits to bariatric surgery, including:
- Improved longevity. Those who undergo bariatric surgery are found to have a lower risk of death than individuals with obesity who have not had surgery.
- Improvement or cure of obesity-related conditions. The majority of patients who have bariatric surgery have an improvement or cure of obesity-related conditions, such as hypertension, diabetes, sleep apnea, asthma, arthritis, and high cholesterol levels.
- Long-term weight loss success. Studies show that more than 90% of people who have bariatric surgery are able to maintain at least 50% of their weight loss following the procedure (Yale Medicine, 2025).
- Increased metabolism. As weight loss occurs, physical activity can increase, such as biking, walking, and swimming, which improves the body’s ability to burn fat efficiently. Hormones like insulin and cortisol are also reduced, which helps lower the body’s storage of fat.
- Improved quality of life. Bariatric surgery patients report a better quality of life after the procedure, including better mobility, reduced depression and anxiety, and improved self-esteem, social interactions, and sexual function (UCI, 2024).
TYPES OF BARIATRIC SURGERY
Bariatric surgical procedures cause weight loss by restricting the volume of food the stomach can hold, causing malabsorption of nutrients, or a combination of the two. They are performed with small incisions using minimally invasive surgical techniques (laparoscopic and robotic surgery).
The goal of the surgical procedures is to modify the stomach and intestines in order to treat obesity and related diseases. The operations may make the stomach smaller and also bypass a portion of the intestine. This results in less intake of food and changes how the body absorbs food for energy, resulting in decreased hunger and increased satiety.
Sleeve gastrectomy and laparoscopic gastric banding are generally considered the safest weight-loss surgeries, with sleeve gastrectomy often having a lower mortality rate and fewer complications compared to gastric bypass (Locket, 2023).
Gastric Bypass (Roux-en-Y)
Gastric bypass is currently the most popular bariatric procedure performed in the United States and is considered the gold standard. The procedure has a restrictive and a malabsorptive component.
The gastric bypass involves dividing the stomach into a smaller pouch on the top (approximately 20 ml in volume) and a larger part below. The lower part of the stomach is bypassed and no longer stores or digests food. The small intestine is also divided and connected to the new stomach pouch to allow food to pass. The small bowel segment which empties the bypassed or larger stomach is connected into the small bowel approximately 3 to 4 feet farther downstream. This results in a bowel connection that resembles the shape of the letter Y.
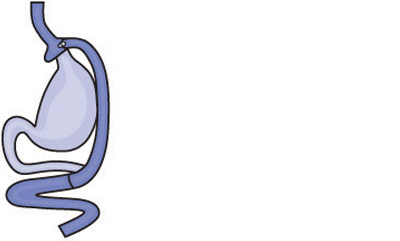
Gastric bypass (Roux-en-Y). (Source: National Institutes of Health.)
Weight loss after a standard 75-cm Roux gastric bypass usually exceeds 100 pounds or about 65%–70% of excess body weight and about 35% of BMI. Longer-limb bypasses are used to obtain comparable weight reductions in patients who have super obesity (BMI >50 kg/m2). Weight loss generally levels off in one to two years, and it is common for patients to regain up to 20 pounds from their weight loss nadir as a long-term plateau (Saber, 2023).
Advantages:
- Fast and dramatic weight loss
- Reliable and long-lasting weight loss
- Effective for remission of obesity-associated conditions
Disadvantages:
- Technically more complex procedure and difficult to reverse
- More vitamin and mineral deficiencies than other procedures
- Risk for small bowel complications and obstruction
- May increase the risk of alcohol and psychiatric disorders
- Risk of developing ulcers, especially with NSAID or tobacco use
A significant risk for this procedure is dumping syndrome, which involves food emptying too rapidly from the stomach into the intestines before it is properly digested. Approximately 85% of people who have this procedure develop some dumping. Symptoms include nausea, bloating, pain, sweating, weakness, and diarrhea and are often triggered by sugary or high-carbohydrate foods (Saber, 2023; Griffin & Vanbuskirk, 2024; Alvarado-Tapias et al., 2023).
Laparoscopic Adjustable Gastric Band
Laparoscopic adjustable gastric banding is a restrictive procedure considered to be one of the least invasive weight-loss surgery options. During this procedure, small incisions are made in the upper abdomen before inserting an adjustable inflatable band around the proximal part of the stomach, creating a small gastric pouch (approximately 15 ml in volume) and a small stoma. When the person eats, this small gastric pouch fills up quickly, making the person feel full more quickly. The food in the small upper pouch will then slowly empty into the main part of the stomach.
The size of the gastric pouch can be adjusted by adding or removing saline from the inflatable band via a reservoir system of saline attached to the band and accessible through a port, which is attached by a catheter to the band. The port is placed subcutaneously in the anterior abdominal wall after the band is secure around the stomach.
Adjustment of the band through the access port is an essential part of this therapy. Appropriate adjustments, performed as often as six times annually, are critical for successful outcomes. The person must chew food thoroughly to allow it to pass through the band. Adjusting the inflation of the cuff changes the size of the opening through which food passes but does not change the size of the gastric pouch. Deflation of the cuff is useful when the outlet is obstructed.
Weight loss following a laparoscopic adjustable gastric banding is about 40%–50% of excess body weight after about two years.
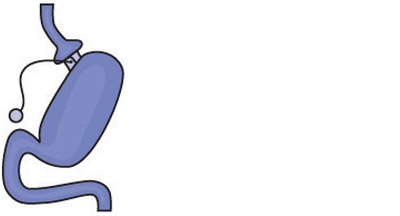
Gastric banding. (Source: National Institutes of Health.)
Advantages:
- Minimally invasive and safter than other weight-loss procedures
- Small scar, fast recovery
- Reversible
- Lower risk of malnutrition than with other surgeries
- Adjustable band
Disadvantages:
- Less dramatic and slower weight loss than with other surgeries
- A 50% chance of complications (e.g., blockage that stops one from being able to eat or problems with the port)
- Band may need several adjustments and monthly office visits during the first year
- Risk of band slippage or damage to the stomach over time (erosion)
- Requires a foreign implant to remain in the body
- Can result in swallowing problems and enlargement of the esophagus
(Saber, 2023; Griffin & Vanbuskirk, 2024)
Gastric Sleeve
Gastric sleeve, also known as vertical sleeve gastrectomy, is a restrictive and malabsorptive procedure that involves removal of 80% of the stomach, leaving a narrow tube or sleeve the size and shape of a banana, which is then connected to the intestines. This restricts the amount of food that can fit in the stomach, creating a feeling of fullness. Decreased appetite results from removal of the part of the stomach that produces the hormones that drive hunger. This surgical procedure is not reversible.
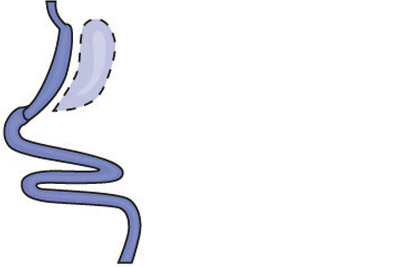
Gastric sleeve. (Source: National Institutes of Health.)
Advantages:
- One of the safest weight-loss surgeries
- Usually performed laparoscopically, resulting in smaller incisions and faster healing
- Can be performed in certain patients with high-risk medical conditions
- Can expect to lose about 60% or more of excess weight in two years
- Does not alter how food is absorbed, resulting in less loss of nutrients
- Can eat a wider range of foods than with other procedures
Disadvantages:
- Nonreversible
- May worsen or cause new-onset esophageal reflux (GERD)
- May produce scar tissue that causes nausea, vomiting, or trouble eating
- May lead to cholelithiasis
- Has less impact on metabolism compared to bypass procedures
- Risk of long-term vitamin deficiencies
(Griffin & Vanbuskirk, 2024)
Biliopancreatic Diversion with Duodenal Switch (BPD-DS)
This is a malabsorption procedure with two components: 1) a surgery similar to the gastric sleeve creates a small tubular stomach pouch, and 2) the duodenum is divided just past the outlet of the stomach. A segment of the distal small intestine is then brought up and connected to the outlet of the newly created stomach pouch, so that when the person eats, food passes through the tube and empties directly into the last segment of the small intestine. This second surgery redirects food to bypass roughly three quarters of the small intestine. The bypassed section is then reattached to the first part of the small intestine, allowing bile and pancreatic enzymes necessary for the breakdown and absorption of protein and fat to mix with food.
Biliopancreatic diversion with duodenal switch. (Source: National Institutes of Health.)
This procedure is more involved than a gastric bypass but can result in even greater and more rapid weight loss. Much of the stomach is removed. However, what remains is larger than the pouches formed during gastric bypass or banding, and larger meals may be eaten with this surgery. The BPD-DS is considered to be the most effective approved metabolic operation for the treatment of type 2 diabetes.
Advantages:
- Results in greater and faster weight loss than gastric bypass or sleeve gastrectomy with the regain of weight
- Affects bowel hormones to cause less hunger and more fullness after eating
- Improves blood sugar control
- Causes less disruption of eating patterns
Disadvantages:
- Slightly higher complication rates than other procedures
- Technically challenging procedure and difficult to reverse
- Highest malabsorption and greater possibility of vitamin and micronutrient deficiencies and dumping syndrome
- Development or worsening of reflux and heart burn
- Risk of looser and more frequent bowel movements
(Saber, 2023; Griffin & Vanburskirk, 2024)
Single Anastomosis Duodenal-Ileal Bypass with Sleeve Gastrectomy (SADI-S)
SADI-S is a simpler form of the duodenal switch. Basically, it’s a sleeve gastrectomy followed by a bypass of the small intestine. It has elements of both restrictive and malabsorptive techniques. This procedure involves the creation of a narrow gastric sleeve by removing about 70%–80% of the stomach, following which a part of the small intestine is rerouted, creating two pathways. One carries food from the stomach to the bowel. The other carries bile from the liver into the small intestine. A smaller stomach results in feeling full with less food. Because the food eaten has less time to mix with digestive acids, fewer calories are absorbed.
Advantages:
- Good weight loss with less hunger, more fullness, blood sugar control, and diabetes improvement
- Simpler and faster to perform than gastric bypass or BPD-DS
- Lower chance of developing a hernia than with biliopancreatic diversion
- Can be performed in those who’ve had a sleeve gastrectomy but have not achieved successful results
Disadvantages:
- Requires diet monitoring and nutritional supplements for the rest of one’s life
- Vitamins and minerals not absorbed as well as with sleeve gastrectomy or gastric band
- Newer procedure with only short-term outcome data
- Potential to worsen or develop new-onset reflux
- Risk of looser and more frequent bowel movements
- Increased flatulence
(Griffin & Vanbuskirk, 2024)
OTHER SURGICAL INTERVENTIONS
Several types of medical devices are approved in the United States for treatment of obesity. One of them may be considered for use in those patients for whom medications are undesirable, ineffective, or not tolerated; for those who are unable or unwilling to undergo bariatric surgery; or as a bridging therapy prior to bariatric surgery. The majority of insurance companies in the United States do not cover the costs of these devices, and the financial burden to the patient may be significant.
- Intragastric balloon systems: Devices inserted into the stomach and expanded with saline (Orbera) or air (Obalon) to produce a sensation of satiety. Intended for weight reduction in conjunction with diet and exercise. Average weight loss with the gastric balloon is about 10% of total weight or about 30% of excess weight.
- Bariatric endoscopy: Involves placement of gastric balloons as well as endoscopic sleeve gastroplasty (a procedure that uses a suturing device that creates a tubular shape similar to the sleeve gastrectomy).
- AspireAssist: Involves a tube running from the inside of the stomach to the outside of the stomach, which allows for drainage of a portion of the stomach’s contents after a meal. This reduces calorie intake by roughly 30%.
(Lockett, 2023)
BARRIERS TO BARIATRIC SURGERY
Bariatric surgery is expensive. Even though patients may spend only two days in the hospital, these operations require the use of expensive, high-technology equipment as well as advanced nursing and surgical training.
The decision to pursue a surgical solution for treatment of obesity is often one taken by middle- to upper-income patients, since most low-income people cannot pay the cost for these procedures.
| (Nevada Surgical, 2024) | |
| Gastric bypass | $20,000 to $35,000 |
| Sleeve gastrectomy | $14,000 to $24,000 |
| Duodenal switch | $23,000 to $30,000 or more |
| Adjustable gastric banding | $14,000 to $20,000 |
| Hospital & facility fees | $5,000 to $15,000 or more |
| Surgeon’s fees | $3,000 to $8,000 or more |
| Pre- and postoperative care | $2,000 to $5,000 |
| Geographic location | Costs higher in metropolitan areas |
Medicare covers some bariatric surgical procedures, such as gastric bypass surgery and laparoscopic banding surgery, when certain conditions are met related to morbid obesity. Medicare does not cover transportation costs to a bariatric surgery center.
Medicaid is a government-sponsored health insurance program for low-income individuals and families. There are 48 states that offer some level of Medicaid coverage for bariatric surgery.
Under the Affordable Care Act, some states require that health insurers selling plans in the marketplace or directly to individuals or small groups cover bariatric surgery. Most major insurance companies will require:
- Proof that surgery or medical intervention is medically necessary
- Completion of a six-month physician-supervised diet program
- Psychological evaluation
- Nutritional evaluation
(Davis, 2024; Nevada Surgical, 2024; Seegert, 2023; Morris, 2024; Medicare.gov, n.d.)
THE ROLES OF OCCUPATIONAL AND PHYSICAL THERAPY IN BARIATRIC SURGERY
Occupational therapists can play a vital role in pre- and postbariatric surgery and bariatric rehabilitation to help patients adopt a healthier lifestyle, increase energy expenditure, improve quality of life, and increase participation in meaningful occupations. Occupational therapy interventions can utilize prevention, health promotion, lifestyle modification, and adaptation approaches for people who have undergone bariatric surgery to restore skills that may have been severely impaired from their prior lifestyle (Tarnowski & Janssen, 2021).
Physical therapists assist in the management of patients who are candidates for bariatric surgery. Therapists help prepare patients for the surgery and recovery by developing and instructing them in individualized pre- and postoperative programs. Preoperatively, therapy may involve strength training and aerobic conditioning. Postoperative programs often begin with deep breathing and lower-extremity exercises to gently increase strength and aerobic conditioning. Physical therapists help patients to minimize pain, regain motion and strength, and return to normal activities as soon as possible (Avruskin, 2021).
CASE
Eric is a 63-year-old man with type 2 diabetes who was referred by his primary care physician to the Kensington Bariatric Center for evaluation for bariatric surgery. The bariatric center is staffed by a team of obesity specialists that includes internists, registered dietitians, nurses, occupational therapists, physical therapists, and a psychologist, all of whom are involved in a comprehensive evaluation of the patient.
Eric’s medical history indicates that his current medications include 70 units of NPH insulin before breakfast and 70 units before dinner, Metformin 850 mg twice a day, atorvastatin, nifedipine, aspirin, and allopurinol. He has sleep apnea but is not currently using his continuous positive airway pressure (CPAP) machine. His reported morning glucose levels are 100–130 mg/dL, hemoglobin A1C level is 6.1% (within normal limits), and his triglyceride level is 201 mg/dL. He weighs 342 pounds, is 5 feet 6 inches tall, and has a BMI of 55.2.
Eric reports that he has experienced obesity since childhood and that he has gained weight every decade since. He is currently at his highest adult weight, and there are no indications that medications or medical complications contribute to his obesity. His family history reveals that his father, two of his sisters, and one of his daughters also have obesity.
Eric describes his past to have included both commercial and supervised medical weight-loss programs. He has been unable to sustain any weight he lost on these programs for more than a few months of discontinuing them. He has been to weight-loss sessions with a registered dietitian and taken part in a hospital-based, dietitian-led, group weight-loss program, where he initially lost weight but then regained it all. He has been on many self-directed diets throughout the years but has never lost any significant weight while on them, and whatever weight he did lose, he once again regained.
A food intake history reveals that Eric eats three meals a day, with dinner being the largest. He sometimes eats between meals, especially if there is food available at his workplace. He eats a snack before bedtime to avoid hypoglycemia. He eats in restaurants once or twice each week but does not frequent any fast-food places. He does not drink alcohol. He admits to binge eating on occasion, even when not hungry, and attributes this to stress.
Eric is a widower who recently began a new relationship. He and his girlfriend have known each other for many years, and she is normal weight. He reports that both he and his girlfriend are concerned about his weight and his diabetes, and he is now willing to consider weight-loss surgery.
Following his evaluation, it is determined that Eric meets the criteria for surgery according to current clinical guidelines because he has clinical severe obesity (BMI ≥40 with comorbid conditions), has failed with less invasive methods of weight loss, and is at high risk for obesity-associated morbidity/mortality. He is found to have no contraindications for surgery.
Eric attends an orientation session where he learns about his surgical options, is given a description of the procedures, including their risks and possible complications, and is encouraged to ask questions. He is referred to the surgeon for evaluation, and it is decided that he will pursue the Roux-en-Y gastric bypass. He is set up for a surgical date and also encouraged to lose weight before the surgery.
Eric does well after surgery, eats without difficulty, and reports feeling no hunger. At two months post surgery, his fasting and pre-dinner blood glucose levels have been consistently less than 120 mg/dL, with no other diabetes medications required.
One year following surgery, Eric’s weight is 254 pounds, a loss of 88 pounds, and he continues to lose weight at approximately 1 to 2 pounds each month. His diabetes, sleep apnea, and hypercholesterolemia are resolved, and his blood pressure is controlled.
MANAGEMENT AND TREATMENT OF OBESITY IN CHILDREN AND ADOLESCENTS
In the cases of childhood obesity, the goal is not to cause weight loss but to reduce the rate of weight gain to fit normal growth curves. The basic principles of management include:
- Modifying diet
- Increasing appropriate physical activity and exercise
- Reducing time spent in sedentary activities
- Modifying behavior
For children who are overweight or with obesity, early treatment is suggested to utilize the highest level of intensity that is appropriate for and available to the individual child.
Management of obesity in children and adolescents also requires family-centered communication and family-based interventions rather than those focused solely on the patient (child or adolescent). Any intervention is likely to fail if it does not involve the active participation and support of family members. Targeting a parent as an important agent of behavior change, either with or without the child, is more effective for long-term weight management than targeting only the child without parental participation. The child may be only one of many family members who have obesity, and successful treatment often requires a change in the entire family’s approach to eating. In selected cases, family therapy may be highly beneficial.
In contrast, a recent study reported that an intensive, group therapy approach was superior to standard, family-based therapy in achieving lifestyle changes and in reducing the BMI of adolescents who are overweight (Hamdy, 2025; Skelton, 2025; Schwarz, 2023).
A team approach to management includes nurse educators, nutritionists, exercise physiologists, and counselors, as well as consultations with pulmonary (sleep) medicine specialists, orthopedists, and gastroenterologists as appropriate. In addition, any acute or chronic complications of obesity are managed, and psychiatric assistance is offered when evidence of psychopathology or dysfunction is present (Schwarz, 2023).
Treatment Models
Intensive Health Behavior and Lifestyle Treatment (IHBLT) is a comprehensive approach to treating obesity among children and adolescents. IHBLT educates and supports families in nutrition and physical activity changes that improve weight status and comorbidities and promote long-term health. IHBLT is most effective when it engages the whole family, occurs face-to-face, and delivers at least 26 hours of nutrition, physical activity, and behavior change lessons over three to 12 months (Hampl et al., 2023).
Comprehensive Obesity Treatment (COT) is a broader framework that encompasses IHBLT and other strategies for managing obesity and related health problems. The essential components of COT for children and adolescents include:
- Treatment of obesity as a chronic disease
- Evaluation and management of comorbidities
- Setting collaborative treatment goals that reflect improvement or resolution of comorbidities, quality of life, self-image
- Integrating weight management components and strategies across appropriate disciplines, which can include intensive health behavior and lifestyle treatment, with pharmacotherapy and metabolic and bariatric surgery if indicated
- Tailoring treatment to the ongoing and changing needs of the individual child or adolescent and the family and community context
(Hampl et al., 2023)
Weight-Loss Goals
The term weight goal is misleading because weight changes as a child grows, and patients may feel discouraged if they do not reach the goal. Throughout the process, counseling instead emphasizes healthy eating patterns and monitors for evidence of disordered eating or distorted body image.
An appropriate focus on weight is a function of the patient’s age and degree of overweight or obesity. For children and adolescents who are overweight or with mild obesity, the goal of maintaining current body weight is appropriate, as this will lead to a decrease in BMI as the child grows taller. If a child is in a phase of rapid linear growth, simply slowing weight gain is more realistic and often improves weight status. For adolescents who have completed linear growth, healthy behaviors, positive body image, and a long-term goal of gradual weight reduction is the focus.
At high degrees of obesity, however, gradual weight loss is safe and appropriate depending on the child’s age and degree of obesity. For children between 2 and 11 years with obesity as well as comorbidities, a weight loss of one pound per month is safe and of benefit but may be difficult to achieve. For adolescents with obesity and comorbidities, it is considered safe to lose up to two pounds per week, although a weight loss of one to two pounds per month is usually a more realistic goal. Because is it difficult to achieve and sustain a dramatic reduction in BMI, realistic goals should emphasize gradual weight loss and maintenance rather than a rapid fall to an ideal body weight (Skelton, 2025).
DIET
For most pediatric patients, highly structured diets—including various forms of balanced low-calorie diets, low-fat diets, low-carbohydrate/low-glycemic index diets, or high-protein diets—should be avoided. While these structured diets may be reasonably effective in achieving short-term weight loss in a motivated patient and are safe if adequately selected and supervised, highly structured diets have poor adherence and success rates over a longer period of time.
Rather than focusing on a specific structured diet, goals are more apt to be achieved if eating behaviors are the focus, and programs that modify family patterns of eating are most likely to be successful.
A semistructured dietary approach is best for weight loss in children, with an aim of encouraging children and families to select food groups with lower energy density and to decrease portion size. Such an approach may include:
- Sitting down together for family meals and avoiding eating in front of a TV, computer, or video game screen, which can lead to fast eating and less awareness of the amount eaten
- Eating the recommended number of fruits and vegetables each day
- Serving whole grain versions of foods, such as whole-wheat bread, whole-grain pasta, and brown rice
- Reducing intake of convenience foods, such as cookies, crackers, fast food, and preprepared meals, which are often high in sugar, fat, sodium, and calories
- Limiting sweetened drinks, including fruit juice
- Serving appropriate portion sizes, starting with a small portion, and allowing children and teens to serve themselves (older children and teens may eat less food when they serve themselves); after finishing a small portion, waiting 10 minutes before taking a second portion
- Not telling a child or adolescent to “clean your plate”
- Serving fat-free or low-fat dairy products and offering nondairy beverages fortified with added calcium, vitamin A, and vitamin D
- Serving lean protein foods; replacing high-fat protein foods like sausage and fried chicken with leaner options, such as turkey breast, beans, or tofu
- Eating breakfast daily
- Avoiding skipping meals
(Mayo Clinic, 2025; Skelton, 2025; NIDDK, 2023)
In circumstances where rapid weight loss is recommended, a protein-sparing modified fast can achieve rapid weight loss in an inpatient or outpatient setting and has been successfully used in children and adolescents with obesity. A high-protein diet, however, does not reduce children’s desire to eat, and ratings of desire to eat significantly have been shown to increase over the duration of such an intervention (Schwarz, 2023).
Weight-loss tools—such as ChooseMyPlate, MyPlate, and HealthyPlate—provide effective visual cues to teach healthy dietary patterns, major food groups, portion sizes, and the goal of including more fruits and vegetables.

(Source: USDA.)
PHYSICAL ACTIVITY
Controlled trials have demonstrated that lifestyle exercise programs, in association with dietary restrictions, provide long-term weight control in children and adolescents. Children should be encouraged to participate in vigorous physical activity throughout adolescence and young adulthood and to limit time spent watching television and videos and playing computer games.
Exercise reduces weight gain through increases in energy expenditure and has favorable effects on cardiovascular status, decreases body fat and total cholesterol levels, increases less body mass and high-density lipoprotein (HDL) levels, and improves psychological well-being.
The guidelines for children and adolescents (ages 6–17) is 60 minutes or more of moderate- to vigorous-intensity physical activity daily, which should include a variety of enjoyable physical activities. As part of those 60 minutes, recommendations call for including the following activities at least three days a week:
- Vigorous activities such as running or soccer
- Activity that strengthens muscles, such as climbing or push-ups
- Activity that strengthens bones, such as gymnastics or jumping rope
(CDC, 2024g)
For children who are school-aged and older, structured physical activity (such as sports or performance arts) is recommended. This may include participation in team or individual sports or supervised exercise sessions. Whether or not a child is willing to engage in structured activities varies, particularly for adolescents. Directly engaging adolescents in choosing activities to replace sedentary time is helpful, as some will enjoy engaging in sports or fitness centers, while others may not (Schwarz, 2023; Skelton, 2025).
For preschool-aged children, most physical activity can be unstructured. Outdoor play is particularly beneficial, as it tends to be active and enjoyed by most children (Skelton, 2025).
The following are recommendations for physical activity in the management of obesity and overweight in children and adolescents:
- Limit screen time. Decrease sedentary behavior such as watching television, surfing the internet, using a tablet or smartphone, and playing video games to no more than two hours per day for children older than 2 years. Children younger than 2 should have no screen time at all.
- Emphasize activity, not exercise. Children should be moderately to vigorously active for at least an hour a day doing activities they enjoy.
(Mayo Clinic, 2025)
DOG OWNERSHIP AND PHYSICAL ACTIVITY
Research has shown that owning a pet, specifically a dog, can significantly impact an individual’s level of physical activity. People with dogs engage in more minutes of physical activity per week and are more than 50% more likely to meet recommended levels of physical activities than people without dogs.
Having a dog in the family will benefit children, too. Children from dog owning households are more physically active, and in one study, young children (5–6 years old) from families with dogs were less likely to be overweight or have obesity (Petfood Institute, 2025).
THE ROLE OF PHYSICAL THERAPY WITH CHILDHOOD OBESITY
The American Physical Therapy Association (2021) recommends that primary care providers involve physical therapists in the management of childhood and adolescent obesity. Physical therapists can assess a child’s risk factors for injury during exercise and evaluate and monitor a child’s increasing level of activity. Recommendations include:
- Do not rely on BMI alone. Use BMI charts that reflect demographics and tools for measuring whole-body fat mass such as waist circumference or skin-fold thickness before beginning treatment. Ideally, it is recommended that body composition be analyzed by cross-sectional imaging.
- Be aware that a child with type 2 diabetes who is receiving insulin treatment can experience hypoglycemia during exercise.
- Evaluate the child’s psychosocial barriers, which may include low self-esteem, anxiety, negative body image, or other psychological issues that can influence how a child will adhere to the plan of care.
- Measure exercise endurance capacity and muscle strength. This can be accomplished by using the 20-meter shuttle run test for endurance and the handgrip strength test and standing broad jump test for muscle strength.
- Promote weight loss by encouraging endurance exercises, whole-body exercises being the best option.
- For children over the age of 5 years, to avoid injury when there is muscle weakness, strength training is recommended under the supervision of a physical therapist to ensure the proper execution of the exercises.
Physical therapists can be very important in helping a child develop a sense of self-efficacy that can motivate them to continue exercising.
CASE
Jaime is a 9-year-old boy who was referred to physical therapy for help in establishing a personal fitness plan after being identified as having obesity during a routine BMI screening at his school. Jaime is a pleasant child who enjoys reading and playing video games during his free time. His dad drives him to and from school, and Jaime spends most of the day in the classroom. At recess, he likes to read on a bench while the other kids play. He attends gym class one day a week.
The physical therapist, Monica, conducted an initial evaluation that included Jaime’s overall health status, history of his current presenting complaint, and screening for medical red flags, as well as evaluation of pain, joint range-of-motion, manual muscle testing, bony and soft-tissue palpation, orthopedic special tests, sensation testing, postural evaluation, gait biomechanics, and static and dynamic balance testing.
Monica next met with Jaime and his parents about an appropriate long-term fitness routine that would include cardiovascular exercise, strength training, flexibility, and functionality work. Jaime looked worried at the mention of exercise. “You won’t make me play basketball, will you?” he whispered. She assured Jaime that there are plenty of exercises he can do that don’t require throwing or catching. Monica helped Jaime and his family plan an activity program designed to gradually increase his activity level to at least 60 minutes/day. His father purchased a stationary bike and a set of free weights for them to use together. Monica reviewed safe weight-lifting technique and set parameters for the appropriate amount of weight for Jaime to be lifting.
Two weeks later, Jaime reported logging 60 minutes of activity on three of seven days and at least 30 minutes on three of the remaining days. His parents also bought him new sneakers and started a daily “family workout night” after dinner, beginning with specific stretches and core strengthening exercises learned at physical therapy, followed by riding the stationary bike or swimming at the community pool. Jaime’s dad started walking to school with him instead of driving. They now log each day’s activities in order to track their progress.
After six weeks, Jaime has made the following progress toward his long-term physical fitness goals:
- A reduced BMI and an absence of weight gain since program initiation
- Reading for half of recess and playing actively with his peers during the other half
- 60 minutes of physical activity attained on 85% of days since the start of the program
Due to the consistent support of Jaime’s parents and his rapid progress toward his physical therapy goals, it is decided that Jaime need not follow up with physical therapy until one month later, at which time he may be discharged to an independent home fitness program.
MENTAL HEALTH ISSUES
Being male, of older age, and affected by severe obesity are most strongly associated with mental health comorbidity in children, adolescents, and young adults with overweight or obesity. Depression, anxiety disorders, eating disorders, and attention-deficit/hyperactivity disorders (ADHD) are more prevalent in children and adolescents with obesity than in healthy-weight youths. The majority of individuals with depression and eating disorders have been found to be females, and ADHD has been found to be higher in males (Galler et al., 2024).
Cognitive behavioral therapy (CBT) emphasizes the process of changing habits and attitudes that maintain psychological disorders and is an appropriate treatment approach for eating disorders and obesity.
Some CBT components include stimulus control to treat impulsivity, goal setting, self-monitoring, stress management, behavioral contracting (rewards), and problem-solving. CBT is beneficial in pediatric populations and post–bariatric surgery patients to improve psychological health and to maintain weight. It can also help with eating disorders, including night eating syndrome, bulimia disorder, and binge eating disorder.
Typical CBT treatments are conducted in 60-minute sessions weekly for eight to 12 weeks. A simple CBT tool is SMART goals (specific, measurable, assignable, realistic, and time-related) (Yearwood & Masood, 2024).
Pharmacology
Pharmacotherapy should be considered for adolescents 12 years and older with severe obesity as an adjunct to diet and physical activity interventions. Evidence shows that medications are effective and generally safe.
The main disadvantages of pharmacotherapy are the need for long-term treatment, with associated costs, and some uncertainty about long-term outcomes. Short-term safety has been established, although information about long-term safety in adolescents is lacking. Considerations for adolescents are described in the table below.
| Drug | Indications |
|---|---|
| (Skelton, 2025; Schwarz, 2023) | |
| Semaglutide (Wegovy), injectable | Indicated as an adjunct to a reduced-calorie diet and increased physical activity for chronic weight management in pediatric patients aged 12 years and older with obesity. Patients should be monitored for depressive symptoms and suicidal thoughts. |
| Liraglutide (Saxenda), injectable | Approved for adolescents ages 12 years and older with obesity. Patients should be monitored for depressive symptoms and suicidal thoughts. Gastrointestinal adverse effects are more common with this medication and can lead to treatment discontinuation. |
| Phentermine (Adipex-P) | Approved for short-term use (12 weeks) in adolescents older than age 16. Long-term study over six months showed modest to moderate effect on BMI, with side effects of increased heart rate and blood pressure. |
| Setmelanotide (Imcivree) | Approved for patients ages 2 years and older to control excess weight caused by rare genetic conditions. |
| Orlistat | Approved for weight loss in adolescents. Causes gastrointestinal side effects that limit its acceptability for many patients. |
| Metformin | An oral diabetic medication used off label in adolescents but with very limited benefits; use in those without type 2 diabetes is questionable. |
Surgical Procedures for Adolescents
Despite robust evidence indicating the safety and efficacy of bariatric surgery, it remains underutilized among the pediatric population. Recommended selection criteria for adolescents younger than 18 years of age include:
- BMI ≥120% of the 95th percentile for BMI for age or BMI ≥35 kg/m2, whichever is lower, with a comorbidity of obesity that has significant effects on health, including but not limited to type 2 diabetes, idiopathic intracranial hypertension, obstructive sleep apnea (apnea-hypopnea index >5), metabolic dysfunction-associated steatohepatitis, Blount disease, slipped capital femoral epiphysis, gastroesophageal reflux disease, arterial hypertension, insulin resistance, or reduced health-related quality of life
- BMI ≥140% of the 95th percentile of BMI for age or BMI ≥40 kg/m2, whichever is lower, with or without an obesity-related comorbidity
or
Contraindications for surgical weight-loss procedures in adolescents include:
- Medically correctable cause of obesity
- Ongoing substance use disorder (within the preceding year)
- Medical, psychiatric, psychosocial, or cognitive condition that prevents adherence to postoperative dietary and medication regimens or impairs decisional capacity
- Current or planned pregnancy within 12 to 18 months of the procedure
- Inability on the part of the patient or parent/guardian to comprehend the risks and benefits of the procedure
(Inge, 2024)
Sleeve gastrectomy (SG), which is a partial gastrectomy, has rapidly increased in use in adolescents over the past decade and now accounts for more than 80% of bariatric procedures in this age group.
Previously, Roux-en-Y gastric bypass (RYGB) surgery was the most commonly performed bariatric procedure but now accounts for less than 20% of procedures in adolescents. RYGB offers some advantage for patients with type 2 diabetes, but there are more risks for nutritional deficiencies compared with a sleeve gastrectomy.
If the patient regains weight in the long term, the sleeve gastrectomy can be converted to a RYGB, but this is uncommon.
Both procedures in adolescents have been shown to lead to clinically important decreases in weight and BMI in the majority of patients in the short to intermediate term (one to three years postoperatively) (Inge, 2024).
CARING FOR THE BARIATRIC PATIENT
Healthcare providers face a number of challenges when working with the growing number of patients with obesity being admitted to hospitals and other healthcare facilities. It is essential that providers understand the physiologic and mobility concerns that may hinder the patient’s capacity to adapt to the stressors of an illness as well as the safety issues for both patients and healthcare workers regarding mobilization.
Respiratory Concerns
Changes in breathing due to obesity include increased respiratory rates, increased oxygen consumption and metabolic requirements, increased work of breathing, and decreased tidal volume. Obesity has a profound effect on the physiology of breathing, leading to pulmonary compromise in a number of ways:
- Decreases in respiratory compliance due to mechanical factors such as increased weight in the thoracic cage and abdomen
- Changes in lung compliance related to the increased pulmonary blood volume
- Disproportionately high percentage of total oxygen consumption for respiratory work, even during quiet breathing, in patients with severe obesity related to decreased lung volumes
- Changes in the airway associated with obstructive sleep apnea, obesity hypoventilation syndrome, and respiratory failure
- Rapid patient oxygen desaturation (hypoxia) due to the decrease in residual volume
Patients with obesity are especially prone to respiratory complications, the most common being obesity-related atelectasis or pneumonia basilar atelectasis, obstructive sleep apnea, and obesity hypoventilation syndrome.
Obesity-related atelectasis or pneumonia basilar atelectasis can occur secondary to the lack of periodic deep breathing. The patient is encouraged to mobilize and to do deep breathing in a sitting or upright position if possible.
Obstructive sleep apnea (OSA) is very common, as obesity seems to increase the passive mechanical pressures, which contributes to upper airway obstruction. This results in repetitive nocturnal oxygen desaturations, fragmented sleep, and excessive daytime somnolence. OSA is commonly treated with continuous positive airway pressure (CPAP) while resting or sleeping.
Hypnotic or narcotic medications should not be administered routinely to patients with obesity, but if such medications are required, patients with OSA must be monitored very closely.
Obesity hypoventilation syndrome (OHS) is characterized by inadequate daytime or nighttime ventilation, resulting in oxygen desaturation and elevated carbon dioxide levels. Patients with OHS often develop heart failure. Acute illness or medications can exacerbate OHS, which presents as decreased level of consciousness due to hypercapnia. The most effective acute treatment is bilevel mask ventilation or bilevel positive airway pressure (BPAP).
Patients are encouraged to practice deep breathing and coughing hourly while awake and to use an incentive spirometer to prevent pneumonia. Lung sounds should be auscultated regularly and the patient observed, particularly at night, for decreased oxygenation with pulse oximetry. Respiratory status is also monitored, as well as nail beds for pallor or cyanosis (AHS, 2022).
Circulation Concerns
Extra weight adds to the risk of high blood pressure and diabetes. Severe obesity can make blood flow through the veins more difficult, increasing the likelihood of varicose veins (twisted and enlarged). Obesity also increases inflammation in the circulatory system.
Obesity is an important risk factor for deep vein thrombosis (DVT) and pulmonary embolism (PE) in both men and women. Atherosclerosis is present 10 times more often in people with obesity compared to those without obesity. Coronary artery disease is also more prevalent because fatty deposits build up in arteries that supply the heart. Narrowed arteries and reduced blood flow to the heart can cause angina or a heart attack. Blood clots can also form in narrowed arteries and cause stroke (Beaumont Health System, 2024; Mandal, 2023).
It is critical to monitor the patient’s cardiac status with consistent and accurate vital signs using an appropriate-sized blood pressure cuff for accuracy. Assessment should include accurate weights, monitoring of edema if present, and capillary refill time of fingers and toes. The patient should be assessed regularly for signs of DVT, including redness, tenderness, or warmth of the lower extremities.
Supine positioning can be dangerous for patients with obesity and should be avoided. When the patient is lying flat, the weight of the panniculus may decrease or impair circulation to the lower extremities. Suitable positions include semi-recumbent and reverse Trendelenburg. For those able to ambulate independently or with assistance, it is recommended they walk as tolerated regularly throughout the day.
Anticlotting medications in combination with sequential compression devices should be considered unless contraindicated. The fit of compression stockings is extremely important, as those that are too small can actually create a tourniquet effect, cutting off circulation in the patient’s lower extremities (AHS, 2022).
Skin Integrity
Because of excess body weight, patients with obesity are predisposed to impairment of skin integrity. Factors that contribute to this include challenges in performing a skin assessment due to difficulty moving and turning the patient and the presence of comorbid conditions such as diabetes, peripheral vascular disease, malnutrition, and lymphedema. Those with obesity may also be at higher risk for skin breakdown related to increased sweating and moisture, possible impaired mobility, increased pressure, and increased shearing during movement.
Adipose tissue has poor blood supply, which leads to inadequate circulation and decreased oxygenation, making the skin vulnerable to breakdown, slower healing, and risk of infections. Potential venous insufficiency can further impair tissue oxygenation.
Increased body size generates more heat, and the body perspires to maintain normal temperature. Excessive sweating increases risk for bacterial and fungal infections in skin folds, especially under breasts and in groin areas.
Skin fold problems occur when there is skin-to-skin contact in which a warm, moist, and dark environment is created, which then increases the potential for skin breakdown, skin-to-skin friction and shear, irritation, rashes, candidiasis, viral or bacterial infection, and potential pressure injuries.
Focus is on the elimination of skin-to-skin contact without causing harm to fragile tissue and on keeping skin folds dry. It is helpful to seek the patient’s input, as they have the most experience in dealing with these skin integrity challenges.
Routine examination of all skin surfaces and skin folds is done daily and increased to every shift if skin is at high risk for breakdown. A validated tool such as the Braden Scale is recommended for skin assessment.
Deep skin folds must be closely monitored, dried thoroughly, and kept open to air as much as possible. Soft, moisture-wicking cloths (such as moisture-wicking textile with antimicrobial silver) between skin folds and antimicrobial and fungus-inhibiting powders are also recommended. The use of cornstarch is not recommended, as is often used in home remedies, since it is a substrate for the growth of yeasts.
Patients with obesity are also at higher risk for pressure injuries, which may include atypical injury, such as between skin folds or under the panniculus. Skin is inspected at least daily for signs of pressure injury, especially nonblanchable erythema. When inspecting darkly pigmented skin, the clinician observes for changes in skin tone, temperature, and tissue consistency compared to skin in other areas of the body.
The patient is turned and repositioned frequently while in bed as well as up in a chair. Equipment may be needed, such as a trapeze to assist with position changes, as well as pressure-relieving devices (AHS, 2022).
Wound Healing
Would healing depends on the circulatory system to provide oxygen and nutrients to damaged tissue. For patients with obesity, adipose tissue is poorly vascularized, and impaired chest expansion results in potential poor oxygenation. The presence of diabetes can further contribute to delayed healing and infections. All phases of wound healing are dependent on adequate supplies of protein, carbohydrates, vitamins, and minerals. Poor nutritional intake can lead to impaired wound healing (AHS, 2022).
General Hygiene and Toileting
Bariatric patients often require access to walk-in bathing facilities, hand-held showerheads, and appropriate-sized shower chairs. Long-handled, soft-bristled shower brushes allow the patient to reach all body areas. Inspection of the skin is done during bathing to determine care needs and interventions.
More frequent bathing is required for patients who are prone to odor problems. Odor may be caused by factors such as incontinence, skin infections, wounds, skin-on-skin contact, and perspiration. Products to manage moisture and odor can be placed in skin folds.
It is not uncommon for patients with obesity to experience urinary incontinence. This can be caused by the pressure on the bladder from a large abdomen or due to skin folds in the perineal area that may impede the voiding process. Incontinence may also result from using the standard, or wrong-sized, bedpan/commode/toilet or from the time it takes to move the patient onto the bedpan or commode.
It is important to ensure that the toilet the patient is using can accommodate their weight. Wall-mounted toilets may not be rated to safely support a person with obesity, and a bariatric commode placed over the toilet may be required.
It is important to ensure that there is enough space in the bathroom to provide the care required if the patient needs assistance with toileting. If staff struggle to move a commode into the bathroom or if they cannot get reasonable access to the patient from the side to perform required care, it may be necessary to use the commode at bedside or in another space with enough room (AHS, 2022).
Medications
Obesity involves many pathophysiologic modifications, such as an increased blood flow and gastrointestinal transit, body composition changes, hepatomegaly, and liver and kidney impairments. These physiologic differences lead to pharmacokinetic changes of drugs, which can significantly impact dosage, clinical tolerance, and efficacy.
When administering and monitoring medications being taken by patients with obesity, clinicians must take into consideration the pharmacokinetic factors described in the table below.
| Stage | Affected by … |
|---|---|
| Absorption |
|
| Distribution |
|
| Metabolism |
|
| Excretion |
|
Almost any class of drug can be affected by the physiologic changes that occur with obesity, but drugs with narrow therapeutic indexes require the most attention. The net effect of this is that both underdosing and overdosing is more likely than with individuals of normal weight, and monitoring of therapeutic levels is important Antibiotics, chemotherapeutic agents, analgesics, anticoagulants, and anticonvulsants are affected by volume and clearance anomalies. It can therefore be challenging to ensure safe therapeutic concentrations for many drugs in these classes (AHS, 2022; Gouju & Legeay, 2023).
Mobility and Safety
Most patients with obesity are at risk for complications related to immobility, and the patient is more at risk of developing these during a long hospitalization. These may include muscle atrophy, constipation, urinary stasis, DVT, atelectasis, pneumonia, pain management problems, cardiac deconditioning, skin breakdown, and depression.
Maintaining the patient’s mobility and safe patient handling pose unique challenges. Patient care areas require equipment designed for patients with obesity. This includes adequate weight-bearing beds, toilets, specialized chairs, and bariatric wheelchairs. Patients may require assistance to transfer out of bed and with ambulation. Care may require additional personnel, proper lifting equipment (such as a ceiling-mounted or portable lift to help reduce the risk of injury to staff), patient and caregiver education, and a standard protocol on the methods of care and use of the equipment.
Lack of appropriate equipment, lack of staff knowledge, and shortage of adequate numbers of caregivers may all be barriers to patient mobility, which increases the complications related to immobility. It is recommended that all staff involved with lifting and transferring patients be knowledgeable and competent to safely transfer patients with bariatric care needs. There is also consensus among patient handling professionals that the goal of safe patient-handling programs should be to eliminate all manual lifting whenever possible.
Before moving a patient, communicate the plan to all involved caregivers, as well as to the patient, and ensure everyone understands their responsibilities. When using a transport chair or wheelchair, make sure the patient is properly positioned before attempting to move them. Use proper body mechanics to prevent injury to self and the patient. Monitor the patient to look for signs of distress or discomfort. Stop the move immediately if the patient encounters discomfort, instability, and worry. Reassess and reassure.
Patients with obesity experience a higher fall rate than the rest of the population. Factors contributing to this include bodyweight distribution, gait disturbance, and overestimation of functional status by the patient. It is important to assess the patient’s ambulation status at least once per day or more often as needed, since the ability of a patient to move in bed, get up and out of bed, and walk about within and outside of the room can vary. It is also essential to support mobility by providing pain management (Ewens et al., 2022; AHS, 2022; Adam, 2024).
GENERAL STRATEGIES FOR OVERWEIGHT AND OBESITY PREVENTION AND ADVOCACY
Every healthcare professional has the opportunity to guide their patients toward making healthy lifestyle choices. Healthcare providers can be role models and bring their knowledge and standing to advocate for healthy changes that connect with people well beyond the healthcare facility they are working in. Every healthcare professional must have the skills to counsel patients about obesity prevention.
Recommendations are provided below for healthcare professionals working with various patient populations in various specialties.
Primary Care Practices
Primary care clinicians play an important role in the assessment, management, and support of patients with obesity. Along with careful clinical assessment and shared decision-making, a flexible treatment plan can be developed that reflects evidence of treatment efficacy, patient preference, and feasibility of implementation (Yanovski & Yanovski, 2024).
With more treatment options becoming available, primary care providers should be equipped and prepared to address obesity within their practices. This multifactorial disease requires a long-term, multifaceted approach. As such, engaging all the relevant stakeholders—including colleagues, ancillary staff, and organizational leadership, as well as community resources—is critical.
Careful attention to the entirety of treatment, from the visit format to clinic setup to addressing implicit bias, allows teams to provide effective, patient-centered obesity treatment in primary care settings (Mulugeta, 2024).
Pediatric Care Practices
The newest research indicates that healthcare interventions in a clinic or office setting in the absence of broader community strategies to prevent obesity may lead to behavior change but may not be adequate to result in sizable improvements in weight. It is therefore recommended that clinic efforts be combined with communitywide changes, such as the Collaborate for Healthy Weight initiative. For all children seen in pediatric offices, recommendations include:
- Measure BMI-percentile-for-age at every well-child visit for children ages 2 years and older; measure weight-for-length percentile for children under 2 years.
- Counsel all patients and families on healthy eating, physical activity, and healthy growth, regardless of current weight status.
- Counsel all patients and families to limit television time to no more than two hours per day and to remove televisions from children’s bedrooms.
- Counsel all patients and families to limit consumption of sugar-sweetened beverages.
- Counsel all patients and families to help children achieve 60 minutes of moderate to vigorous physical activity per day.
- Establish procedures for follow-up assessment (including laboratory tests), counseling, and treatment plans for children who are overweight or with obesity.
- Establish policies to avoid weight bias in pediatric clinics, which may include requiring all employees to be trained on weight-bias prevention.
(Skelton, 2025; Harvard T.H. Chan, 2022)
Obstetrical Care Practices
There are many factors before and during pregnancy that can affect a child’s obesity risk later in life. The following recommendations pertain to obstetrical care practices:
- At the first prenatal visit, BMI is calculated and a recommendation made about the amount of weight that should be gained throughout pregnancy.
- Behavioral interventions using diet and exercise are recommended and have been shown to help reduce gestational weight gain in pregnant patients with overweight and obesity.
- A patient should be counseled appropriately during a preconception visit on achieving a healthy weight through balanced nutrition and physical activity.
- By optimizing the body weight and metabolic environment prior to pregnancy, insulin resistance, inflammation, oxidative stress, and lipotoxicity associated with obesity can be reduced, and the adverse effects to the mother and the fetus can be minimized.
- Early screening and management of obesity in pregnancy can help improve overall outcomes. Referrals to specialists such as endocrinology, dietitian, or weight management can also be considered when deemed appropriate.
(Kim & Ayabe, 2023)
Hospital and Clinic Efforts
The following are recommendations for helping in the prevention of obesity in hospital settings:
- Encourage healthcare providers to model healthy eating.
- Create incentive-based physical activity programs for employees.
- Initiate employee wellness programs that include promoting use of stairs and walking trails.
- Offer healthy foods and beverages to employees and patients.
- Ban the sale and marketing of unhealthy foods and beverages on clinic and hospital premises.
- Promote breastfeeding for infants born in the hospital or clinic, as well as for hospital and clinic employees who are nursing.
(Harvard T.H. Chan, 2022)
Schools
Schools can implement policies and practices that encourage healthy eating and physical activity during the school day, and can also help children and adolescents establish lifelong healthy patterns. This is especially important for children from households with lower incomes and children who are members of racial/ethnic minority groups (who, on average, have less access to healthy food, poorer dietary quality, and higher risk for obesity compared to other children) (Harvard T.H. Chan, 2022).
Ending Weight Stigma in Healthcare
Substantial evidence demonstrates the widespread experiences and impact of weight stigma that is ultimately leading to inequitable healthcare for those living with obesity. The overwhelming evidence that such weight stigma in healthcare is detrimental must be addressed. Some strategies recommended by the Joint International Consensus Statement for ending the stigma include:
- Increasing personal awareness
- Recognizing the complexity of obesity as a chronic disease rather than personal choice
- Placing a greater focus on health instead of weight
- Using person-first language, for example, “a patient with obesity” instead of “an obese patient”
- Using nonstigmatizing images in patient education and other literature
- Treating individuals with obesity with dignity and respect
Ending obesity bias, stigma, and discrimination begins with awareness and acknowledgment of both individual beliefs and of obesity as a complex chronic disease of energy dysregulation. Creating a culture of inclusion and belonging must be expanded to include acceptance of all people at all weights without judgment or discrimination (Trout, 2023).
Barriers to the Provision of Weight Management in Primary Care Clinics
The current outcomes of obesity treatment indicate a failure of both patients and physicians in initiating or maintaining interventions. Recent studies have been done to identify and understand the barriers to obesity management in clinical settings from the points of view of both patients and healthcare providers.
Despite healthcare providers’ opportunity to help patients with obesity achieve weight loss, many face challenges that hinder their ability to provide evidence-based obesity treatment.
- Healthcare providers (HCPs) cite limited appointment time for patient visits as the main reason for not discussing weight management with their patients.
- Insufficient knowledge, training, and counseling skills for obesity make it difficult for HCPs to provide counseling for obesity. Obesity education for HCPs includes diverse fields such as diet, nutrition, exercise, behavior therapy, and medication. Medical schools are urged to adequately address obesity education in their curricula.
- When HCPs do provide counseling for weight management, it often consists only of general advice on diet and physical activity without specific, evidence-based treatment or follow-up plans.
(Oshman et al., 2023)
The main barrier patients report to having discussions about weight issues and management with their healthcare provider is feeling judged and blamed for their weight. Other factors include:
- Lower trust in providers
- Poorer provider–patient communication
- Reduced quality of care
- Inadequate medical equipment to accommodate patients of diverse body sizes
- Poorer treatment outcomes
- Avoidance and delay of care
(Puhl, 2023)
CONCLUSION
Obesity around the world and in the United States continues to be a major problem. Researchers have learned a great deal over the past several years about the pathogenesis and contributing factors involved in the development of obesity and, as a result, have a much better understanding of this chronic disease. However, despite these efforts, the problem persists and continues to grow.
Of great concern is the need for healthcare providers to become aware of their own biases and the socially accepted stigma surrounding overweight and obesity, similar to efforts regarding issues of mental health. Overweight and obesity require healthcare professionals to take an active role in the prevention of obesity and treatment for those who live with this disease and to learn that compassion, empathy, and patience are necessary to become a positive force against this modern public health concern.
RESOURCES
Adult obesity facts (CDC)
BMI calculator (U.S. DHHS)
Institute for Healthy Childhood Weight (American Academy of Pediatrics)
Obesity (CDC)
Pediatric growth charts (CDC)
REFERENCES
Adam. (2024). How to move a bariatric patient safely. https://designspecific.co.uk/how-to-move-a-bariatric-patient-safely/
Alberta Health Services (AHS). (2022). Guidelines for the care of hospitalized patients with bariatric care needs. https://www.albertahealthservices.ca/assets/about/scn/ahs-scn-don-guidelines-for-hospitalized-patients-bariatric-needs.pdf
Allied Digestive Health. (2024). How obesity affects your gut health. https://allieddigestivehealth.com/how-obesity-affects-your-gut-health/
Alomare J. (2024). The 5 principles of motivational interviewing: A guide to empowering change. https://relevancerecovery.com/blog/the-5-principles-of-motivational-interviewing-a-guide-to-empowering-change/
Alvarado-Tapias E, Marti-Aguado D, Kennedy K, et al. (2023). Bariatric surgery is associated with alcohol-related liver disease and psychiatric disorders associated with AUD. Obes Surg, 33(5), 1494–1505.
American Association for Clinical Chemistry (AACC). (2022). Lipid profile. Testing.com. https://www.testing.com/tests/lipid-panel/
American Association of Clinical Endocrinologists. (AACE). (n.d.). What is the disease of obesity? Clinical evaluation. https://slideplayer.com/slide/13179111/
American Physical Therapy Association (APTA). (2021). Physical therapist’s guide to obesity. https://www.choosept.com/guide/physical-therapy-guide-obesity
American Society for Metabolic and Bariatric Surgery (ASMBS). (2024a). Disease of obesity. https://asmbs.org/patients/disease-of-obesity/
American Society for Metabolic and Bariatric Surgery (ASMBS). (2024b). Is metabolic and bariatric surgery right for you? https://asmbs.org/patients/is-metabolic-and-bariatric-surgery-right-for-you/
American Thyroid Association (ATA). (2024). Thyroid and weight. https://www.thyroid.org/thyroid-and-weight/
Anderson L. (2025). Side effects of weight loss drugs (diet pills). https://www.drugs.com/article/side-effects-weight-loss-drugs.html
Arrona-Cardoza P, Labonte K, et al. (2023). The effects of food advertisements on food intake and neural activity: A systematic review and meta-analysis of recent experimental studies. Advances in Nutrition, 14(2), 339–51.
Avruskin A. (2021). Physical therapy guide to obesity. Choose PT. https://www.choosept.com/guide/physical-therapy-guide-obesity
Bahinipati J, Sarangi R, Pathak M, & Mohapatra S. (2022). Effect of night shift on development of metabolic syndrome among health care workers. J Family Med Prim Care, 11(5), 1710–15.
Baile JI, González-Calderón MJ, & Rabito-Alcón MF. (2022). Obesity bias in the school setting: A brief report. Children (Basel), 9(7), 1067.
Balasundaram P & Krishna S. (2023). Obesity effects on child health. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK570613/
Beaumont Health System. (2024). Health effects of obesity. https://www.beaumont.org/conditions/obesity-and-heart-disease
Beal V. (2024). Fitness tracker. https://www.techopedia.com/definition/fitness-tracker
Bleistein A. (2022). From the Obesity Medicine Association: The alarming link between screen time and pediatric obesity. https://www.physiciansweekly.com/from-the-obesity-medicine-association-the-alarming-link-between-screen-time-pediatric-obesity
Brezinski D. (2024). How chronic inflammation may contribute to body weight. https://www.drbnaples.com/link-between-inflammation-and-weight/
Burridge K, Christensen S, Golden A, et al. (2022). Obesity history, physical exam, laboratory, body composition, and energy expenditure: An Obesity Medicine Association clinical practice statement, 2022. Obesity Pillars, 1, 100007. https://doi.org/10.1016/j.obpill.100004
Calculator Academy Team. (2024). RFM calculator (relative fat mass). https://calculator.academy/rfm-calculator-relative-fat-mass/
Centers for Disease Control and Prevention (CDC). (2024a). New CDC data show adult obesity prevalence remains high. https://www.cdc.gove/media/releases/2024/p0912-adult-obesity.htm
Centers for Disease Control and Prevention (CDC). (2024b). Diabetes during pregnancy. https://www.cdc.gov/maternal-infant-health/pregnancy-diabetes/index.html
Centers for Disease Control and Prevention (CDC). (2024c). Breastfeeding report card. https://www.cdc.gov/breastfeeding/data/reportcard.htm
Centers for Disease Control and Prevention (CDC). (2024d). BMI frequently asked questions. https://www.cdc.gov/bmi/faq/
Centers for Disease Control and Prevention (CDC). (2024e). Adult BMI categories. https://www.cdc.gov/bmi/adult-calculator/bmi-categories.html
Centers for Disease Control and Prevention (CDC). (2024f). Child and teen BMI calculator. https://www.cdc.gov/bmi/child-teen-calculator/bmi-categories.html
Centers for Disease Control and Prevention (CDC). (2024g). What you can do to meet physical activity recommendations. https://www.cdc.gov/physical-activity-basics/guidelines/index.htm
Centers for Disease Control and Prevention (CDC). (2023a). 2023 adult obesity prevalence map. https://www.cdc.gov/obesity/data-and-statistics/adult-obesity-prevalence-maps.html
Centers for Disease Control and Prevention (CDC). (2023b). Physical activity and your weight and health. https://www.cdc.gov/healthy-weight-growth/physical-activity/index.htm
Cheng S, Kaminga A, Liu Q, et al. (2022). Association between weight status and bullying experiences among children and adolescent in schools: An updated meta-analysis. Child Abuse & Neglect, 134, 105833.
Ciezju S, Odyiewska E, Bossowski A, & Glowinska-Olszewska B. (2024). Not only metabolic complications of childhood obesity. Nutrients, 16(4), 539.
Cleveland Clinic. (2024). What you need to know about the Ornish diet. https://health.clevelandclinic.org/ornish-diet
Cleveland Clinic. (2023). Gut microbiome. https://my.clevelandclinic.org/health/body/25201-gut-microbiome
Cleveland Clinic. (2022a). Leptin. https://my.clevelandclinic.org/health/articles/22446-leptin
Cleveland Clinic. (2022b). Is BMI an accurate measure of health? https://health.clevelandclinic.org/is-bmi-accurate/
Colleluori G & Villareal DT. (2022). Weight strategy in older adults with obesity: Calorie restriction or not? Curr Opin Clin Nutr Metab Care, 26(1), 17–22.
CORE Institute. (2024). Carrying extra pounds: How weight affects your bones, joints, and mobility. https://thecoreinstituteaz.com/carrying-extra-pounds-how-weight-affects-your-bones-joints-and-mobility/
Crane M, Newman K, Appelhans B, et al. (2022). Weight loss program preferences of men working in blue-collar occupations: A qualitative inquiry. American Journal of Men’s Health, 16(5). https://journals.sagepub.com/doi/10.1177/15579883221117932
Cunningham M. (2024). Social and structural factors are key drives of disparities in obesity rates. https://publichealth.gmu.edu/news/2024-08/social-and-structural-factors-are-key-drivers-disparities-obesity-rates
Davis J. (2024). Paying for weight loss surgery. WebMD. https://www.webmd.com/obesity/financing-weight-loss-surgery
Delta College. (2024). Live health? Exercise and fitness. http://library.delta.edu/c.php?g=1108756&p=8087080
Dietz W. (2024). Weight discrimination in the workplace. https://stop.publichealth.gwu.edu/LFD-apr24
Dietz W. (2023a). The economic impact of obesity. https://stop.publichealth.gwu.edu/LFD-oct23
Dietz W. (2023b). Prescription medications and weight gain. https://stop.publichealth.gwu.edu/LFD-mar23
DiLonardo M. (2024). The connection between sleep and obesity. https://www.webmd.com/sleep-disorders/sleep-obesity
Dowgiatto-Gornowicz N, Lech P, & Major P. (2023). Bariatric and metabolic surgery in patients older than 65 years—A multicenter study. Obes Surg, 33(10), 3106–11.
Easy Sociology. (2024). Exploring the connections between ethnicity and food insecurity: The sociology perspective. https://easysociology.com/sociology-of-culture/sociology-of-food/exploring-the-connections-between-ethnicity-and-food-insecurity-the-sociology-perspective/
Ellis D. (2023). Is night shift work rewiring our appetite and driving weight gain? https://www.news-medical.net/news/20231010/Is-night-shift-work-rewiring-our-appetite-and-driving-weight-gain.aspx
Ewens B, Kemp V, Towell-Barnard A, & Whitehead L. (2022). The nursing care of people with Class III obesity in an acute care setting: A scoping review. BMC Nurs, 21, 33. https://doi.org/10.1186/s12912-021-00760-7
Feng Z, Fang C, Ma Y, et al. (2024). Obesity-induced blood–brain barrier dysfunction: Phenotypes and mechanisms. J Neuroinflammation, 21, 110. https://doi.org/10.1186/s12974-024-03104-9dysfunction: phenotypes and mechanisms
Fletcher J. (2023). What can you eat on a low-carb diet? https://www.medicalnewstoday.com/articles/321545#low-carb-foods
Franco-Pérez J. (2024). Mechanisms underlying memory impairment induced by fructose. Neuroscience, 548, 27–38.
Frey M. (2024). A high-protein diet: Is it right for you. https://www.verywellfit.com/is-a-high-protein-diet-best-for-weight-loss-3495768
Fulton M & Srinivasan V. (2023). Obesity, stigma and discrimination. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK554571/
Galler A, Thönnes A, Joas J, et al. (2024). Clinical characteristics and outcomes of children, adolescents and young adults with overweight or obesity and mental health disorders. Int J Obes, 48, 423–32. https://doi.org/10.1038/s41366-023-01449-4
Ge L, Sadeghirad B, Ball G, et al. (2020). Comparison of dietary macronutrients patterns of 14 popular named dietary programmes for weight and cardiovascular risk factor reduction in adults: Systematic review and network meta-analysis of randomized trials. BMJ, 1(369), 696.
Geng J, Qingqiang N, Sun W, et al. (2022). The links between gut microbiota and obesity and obesity related diseases. Biomedicine & Pharmacotherapy, 147, 112678. https://doi.org/10.1016/j.biopha.2022.112678
Godoy M. (2023). What we know about the health risks of ultra-processed foods. https://www.npr.org/sections/health-shots/2023/05/25/1178163270/ultra-processed-foods-health-risk-weight-gain
Goodman B. (2023). Food addiction. WedMD. https://www.webmd.com/mental-health/eating-disorders/binge-eating-disorder/mental-health-food-addiction
Gouju J & Legeay S. (2023). Pharmacokinetics of obese adults: Not only an increase in weight. Biomedicine & Phamacotherapy, 166, 115281. https://doi.org/10.1016/j.biopha.2023.115281
Griffin RM & Vanbuskirk S. (2024). Choosing a type of weight loss surgery. WedMD. https://www.webmd.com/obesity/weight-loss-surgery-making-the-choice
H & S Crew. (2024). The hidden link between seed oils and chronic disease. https://heartandsoil.co/blog/seed-oils-and-chronic-disease
Hamdy O. (2025). Obesity treatment & management. Medscape. https://emedicine.medscape.com/article/123702-overview
Hampl S, Hassink S, Skinner A, Armstrong S, et al. (2023). Clinical practice guideline for the evaluation and treatment of children and adolescents with obesity. Pediatrics, 151(2), e2022060640. https://doi.org/10.1542/peds.2022-060640
Harvard T.H. Chan School of Public Health. (2025). Physical activity. https://nutritionsource.hsph.harvard.edu/physical-activity-research/
Harvard T.H. Chan School of Public Health. (2022). Healthcare obesity prevention recommendations: Complete list. https://www.hsph.harvard.edu/obesity-prevention-source/obesity-prevention/healthcare/healthcare-obesity-prevention-recommendations-complete-list/
Hayden M, Dixon M, Dixon J, Playfair J, & O’Brien P. (2010). Perceived discrimination and stigmatization against severely obese women: Age and weight loss make a difference. Obes Facts, 3, 7–14. https://doi.org/1159/00027320
Inge T. (2024). Surgical management of severe obesity in adolescents. UpToDate. https://www.uptodate.com/contents/surgical-management-of-severe-obesity-in-adolescents
Johns Hopkins Medicine. (2025a). Does the time of day you eat matter? https://www.hopkinsmedicine.org/health/wellness-and-prevention/does-the-time-of-day-you-eat-matter
Johns Hopkins Medicine. (2025b). Intermittent fasting: What is it, and how does it work? https://www.hopkinsmedicine.org/health/wellness-and-prevention/intermittent-fasting-what-is-it-and-how-does-it-work
Johnston B. (2024). Zepbound (tirzepatide)—Uses, side effects, and more. WebMD. https://www.webmd.com/drugs/2/drug-187794/zepbound-subcutaneous/details
Jones BL, Orton AL, et al. (2023). Barriers to healthy family dinners and preventing child obesity: Focus group discussions with parents of 5-to-8-year-old children. Children (Basel), 10(6), 952. https://doi.org/10.3390/children10060952
Kalinderi K, Goula V, Sapountzi E, et al. (2024). Syndromic and monogenic obesity: New opportunities due to genetic-based pharmacological treatment. Children, 11(2), 153.
Khanna D, Welch B, & Rehman A. (2024). Pathophysiology of obesity. StatPearls Publishing. https://pubmed.ncbi.nlm.nih.gov/34283442/
Kim H & Ayabe A. (2023). Obesity in pregnancy. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK572113/
Kokka L, Mourikis I, & Bacopoulou F. (2023). Psychiatric disorders and obesity in childhood and adolescence—A systematic review of cross-sectional studies. Children (Basel), 102, 285.
Leach L, Doan T, & Strazdins D. (2023). Working longer hours and body weight: An Australian study using household panel data (with measures of paid and unpaid time) to provide gender-specific estimates. SSM Population Health, 24, 101561.
Lee K, Arriola-Sanchez L, Lumeng J, Gearhardt A, & Tomiyama A. (2022). Weight stigma by association among parents of children with obesity: A randomized trial. Aced Pediatr, 22(5), 754–60.
Leech J. (2023). High-fructose corn syrup: Just like sugar, or worse? https://www.healthline.com/nutrition/high-fructose-corn-syrup-vs-sugar
Leth-Møller M, Kampmann U, Hede S, et al. (2024). The association of fetal growth rate and growth in first year of life with childhood overweight: A cohort study. Int J Obes, 48, 1822–30.
Levy S & Nessen M. (2023). Obesity. https://www.msdmanuals.com/professional/nutritional-disorders/obesity-and-t
Lily B. (2024). Body positivity and mental wellness: Embracing self-love. https://www.tanner.org/the-scope/body-positivity-and-mental-wellness-embracing-self-love
Lim Y & Boster J. (2024). Obesity and comorbid conditions. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK574535/
Lockett E. (2023). Your guide to weight loss procedures without surgery. https://www.healthline.com/health/diet-and-weight-loss/weight-loss-procedures-without-surgery
Loma Linda University (LLU). (2025). Stages of change model. https://medicine.llu.edu/academics/resources/stages-change-model
Lyun O, Okobi O, Nwachukwu E, Miranda W, et al. (2024). Analyzing obesity trends in American children and adolescents: Comprehensive examination using the National Center for Health Statistics (NCHS) Database. Cureus, 16(6), e61825. https://doi.org/10.7759/cureus.61825
MacMillan C. (2024). Ultraprocessed foods: Are they bad for you? https://www.yalemedicine.org/news/ultraprocessed-foods-bad-for-you
Mallik R, Carpenter J, & Zalin A. (2023). Assessment of obesity. Clin Med (London), 23(4), 299–303.
Mandal A. (2023). Obesity and deep vein thrombosis (DVT). https://www.news-medical.net/health/Obesity-and-deep-vein-thrombosis-(DVT).aspx
Marshall L. (2023). Excess weight, obesity more deadly than previously believed. https://www.colorado.edu/today/2023/02/23/excess-weight-obesity-more-deadly-previously-believed
Martinelli LA. (2022). Stakeholders and ethics in healthcare: Ethical accountability for organizations. https://www.google.com/books/edition/_/ShekzgEACAAJ?hl=en
Marti-Nicolovius M. (2022). Effects of overweight and obesity on cognitive functions of children and adolescents. Rev Neuro, 75(3), 59–65.
Masood B & Moorthy M. (2023). Causes of obesity: A review. Clinical Medicine, 34(4), 284–91.
Mayo Clinic. (2025). Childhood obesity. https://www.mayoclinic.org/diseases-conditions/childhood-obesity/diagnosis-treatment/drc-20354833
Mayo Clinic. (2023a). Cushing syndrome. https://www.mayoclinic.org/diseases-conditions/cushing-syndrome/symptoms-causes/syc-20351310
Mayo Clinic. (2023b). Stress management. https://www.mayoclinic.org/healthy-lifestyle/stress-management/in-depth/stress/art-20046037
Mayo Clinic. (2023c). Obesity. https://www.mayoclinic.org/diseases-conditions/obesity/diagnosis-treatment
Mayo Clinic. (2023d). DASH diet: Healthy eating to lower your blood pressure. https://www.mayoclinic.org/healthy-lifestyle/nutrition-and-healthy-eating/in-depth/dash-diet/art-20048456
Mayo Clinic. (2022). Prescription weight-loss drugs. https://www.mayoclinic.org/healthy-lifestyle/weight-loss/in-depth/weight-loss-drugs/art-20044832
Medicare.gov. (n.d.). Bariatric surgery. https://www.medicare.gov/coverage/bariatric-surgery
Mersch J. (2025). Pediatric vital signs ranges and charts. https://www.emedicinehealth.com/pediatric_vital_signs/article_em.htm
Michalowska J. (2024). RFM calculator (relative fat mass). https://www.omnicalculator.com/health/relative-fat-mass
Migala J. (2024). The 10 most famous fad diets of all time. https://www.everydayhealth.com/food/the-10-most-famous-fad-diets-of-all-time.aspx
Morris M. (2024). Does Medicaid cover weight-loss surgery. https://www.goodrx.com/insurance/medicaid/weight-loss-surgery-medication-coverage
Mulugeta W. (2024). Integrating weight management in primary care. https://info.primarycare.hms.harvard.edu/perspectives/articles/integrating-weight-management-in-primary-care
Muntefering C, Fields B, & Christensen J. (2023). Going beyond management and maintenance: Occupational therapy’s role in primary prevention for adults at risk of obesity. American Journal of Occupation Therapy, 77(5), 7705347020.
Murdock J. (2024). The latest updates: 16 new weight loss drugs on the horizon. https://www.goodrx.com/conditions/weight-loss/new-weight-loss-drugs
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). (2024). Prescription medications to treat overweight & obesity. https://www.niddk.nih.gov/health-information/weight-management/prescription-medications-treat-overweight-obesity
National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). (2023). Helping your child who is overweight. https://www.niddk.nih.gov/health-information/weight-management/helping-your-child-who-is-overweight
National Institute of Environmental Health Sciences (NIEHS). (2024a). Obesity. https://www.niehs.nih.gov/health/topics/conditions/obesity/index.cfm
National Institutes of Health (NIH). (n.d.). Therapeutic lifestyle changes (TLC) to lower cholesterol. https://www.nhlbi.nih.gov/education/TLC-Therapeutic-Lifestyle-Changes-Lower-Cholesterol
National Institutes of Health (NIH). (2024a). Carpenter syndrome. https://rarediseases.info.nih.gov/diseases/6003/carpenter-syndrome
National Institutes of Health (NIH). (2024b). Down syndrome. https://medlineplus.gov/downsyndrome.html
National Institutes of Health (NIH). (2023a). Screen time and children. https://medlineplus.gov/ency/patientinstructions/000355.htm
National Institute of Health (NIH). (2023b). Circadian rhythms. https://www.nigms.nih.gov/education/fact-sheets/Pages/circadian-rhythms.aspx
National Organization for Rare Disorders (NORD). (2023a). Beckwith-Wiedemann syndrome. https://rarediseases.org/rare-diseases/beckwith-wiedemann-syndrome/
National Organization for Rare Disorders (NORD). (2023b). Cohen syndrome. https://rarediseases.org/rare-diseases/cohen-syndrome/
National Organization for Rare Disorders (NORD). (2022). Hypothalamic obesity, acquired. https://rarediseases.org/rare-diseases/hypothalamic-obesity-acquired/
Nelson C. (2023). The 4 types of parenting styles: What style is right for you? https://mcpress.mayoclinic.org/parenting/what-parenting-style-is-right-for-you
Nevada Surgical. (2024). How much does bariatric surgery cost? https://nevadasurgical.com/bariatric-surgery/how-much-does-bariatric-surgery-cost/>
Newsom R & Rehman A. (2024). The connection between diet, exercise, and sleep. Sleep Foundation. https://www.sleepfoundation.org/physical-health/diet-exercise-sleep
Nguyen Q, Tasdizen T, Alirezaek M, et al. (2024). Neighborhood built environment, obesity and disease: A Utah siblings study. SSM Population Health, 26, 101670.
Niemiro G, Rewane A, & Algotar A. (2023). Exercise and fitness effect on obesity. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK539893
Nuesana. (2024). The impact of work stress on obesity and metabolic syndrome. https://nuesana.com/the-impact-of-work-stress-on-obesity-and-metabolic-syndrome/
Nunez K. (2024). 12 exercises that burn the most calories. https://www.healthline.com/health/what-exercise-burns-the-most-calories#calorie-burning-exercises
Obesity Action Coalition (OAC). (2025). Understanding obesity stigma brochure. https://www.obesityaction.org/get-educated/public-resources/brochures-guides/understanding-obesity-stigma-brochure/
Obesity Evidence Hub (OEH). (2023). Impact of unhealthy food marketing on children. https://www.obesityevidencehub.org.au/collections/prevention/the-impact-of-food-marketing-on-children
Obesity Medicine Association (OMA). (2023a). Motivational interviewing for obesity treatment. https://obesitymedicine.org/blog/motivational-interviewing/
Obesity Medicine Association (OMA). (2023b). What is obesity? https://obesitymedicine.org/blog/what-is-obesity/
Ogle S, Schmoke N, & Inge T. (2025). Adolescent bariatric surgery. Endotext. https://www.ncbi.nlm.nih.gov/books/NBK575728/
Oh R, Gilani B, & Uppaluri K. (2023). Low-carbohydrate diet. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK537084/
Ohri-Vachasapti P, Acciai F, Melnick E, et al. (2023). Food environments within and outside of schools play a critical role in curtailing the rise in obesity among school-aged children over time. Journal of Nutrition, 153(12), 2565–75.
Oshman L, Othman A, Furst W, et al. (2023). Primary care providers' perceived barriers to obesity treatment and opportunities for improvement: A mixed methods study. Plos One, 18(4), e0284474.
Perreault L. (2023). Determining body composition in adults. UpToDate. http://114.255.80.174:8084/contents/determining-body-composition-in-adults
Perreault L & Burgermaster M. (2024). Obesity in adults: Behavioral therapy. UpToDate. https://www.uptodate.com/contents/obesity-in-adults-behavioral-therapy
Perreault L & Delahanty L. (2024). Obesity in adults: Dietary therapy. UpToDate. https://www.uptodate.com/contents/obesity-in-adults-dietary-therapy
Perreault L & Laferrère B. (2024). Overweight and obesity in adults: Health consequences. UpToDate. https://www.uptodate.com/contents/overweight-and-obesity-in-adults-health-consequences/contributors
Perreault L & Reid T. (2024). Obesity in adults: Drug therapy. UpToDate. https://www.uptodate.com/contents/obesity-in-adults-drug-therapy?topicRef=5382&source=see_link
Perreault L & Rosenbaum M. (2024). Obesity: Genetic contribution and pathophysiology. UpToDate. https://www.uptodate.com/contents/obesity-genetic-contribution-and-pathophysiology
Petfood Institute. (2025). Physical health benefits of pets. https://www.petfoodinstitute.org/physical-health-benefits-of-pets/
Phillips S & Shulman R. (2023). Measurement of body composition in children. UpToDate. https://www.uptodate.com/contents/measurement-of-body-composition-in-children#H14
Physicians Premiere. (2023). Can shift work cause you to gain weight? https://healthymeweightloss.com/blogs/can-shift-work-cause-you-to-gain-weight/
Physiopedia. (2025a). Physical activity and the built environment. https://www.physio-pedia.com/Physical_Activity_and_the_Built_Environment#
Physiopedia. (2025b). Management of obesity. https://www.physio-pedia.com/Management_of_Obesity
Puhl RM. (2023). Weight stigma and barriers to effective obesity care. Gastroenterol Clin N Am, 52(2), 417–28. https://doi.org/10.1016/j.gtc.2023.02.002
Ramsey P & Schenken R. (2024). Obesity in pregnancy: Complications and maternal management. UpToDate. https://www.uptodate.com/contents/obesity-in-pregnancy-complications-and-maternal-management
Ratini M. (2023). What to know about obesogens. WebMD. https://www.webmd.com/obesity/what-to-know-obesogens
Research Features. (2023). How opioids drive our salt consumption. https://researchfeatures.com/how-opioids-drive-salt-consumption/
Rogers K. (2024). Adipose tissue. https://www.britannica.com/science/adipose-tissue
Ross F, Patangia D, Grimaud G, et al. (2024). The interplay between diet and the gut microbiome: Implications for health and disease. Nature Reviews Microbiology, 22, 671–86.
Saber A. (2023). Bariatric surgery treatment and management. Medscape. https://emedicine.medscape.com/article/197081-treatment#d10
Saeed S, Bonnefond A, & Froguel P. (2025). Obesity: Exploring its connection to brain function through genetic and genomic perspectives. Mol Psychiatry, 30, 651–8. https://doi.org/10.1038/s41380-024-02737-9
Sampson K. (2023). What is the gold standard for determining body fat? https://obesitymedicine.org/blog/what-is-the-gold-standard-for-determining-body-fat
Sanches M, Goldberg T, Rizzo A, da Silva V, et al., (2023). Inflammatory cytokines and chemokines in adolescents with antibody against adenovirus 36. Sci Rep 13, 9918. https://doi.org/10.1038/s41598-023-33084-4
Savulescu-Fiedler I, Mihalcea R, Dragosloveanu S, et al. (2024). The interplay between obesity and inflammation. Life (Basel), 14(7), 856. https://doi.org/10.3390/life14070856
Scarpelli DG, Burrows W, et al. (2025). Disease. Brittanica. https://www.britannica.com/science/disease
Schnurr T, Ängquist L, Nøhr E, et al. (2022). Smoking during pregnancy is associated with child overweight independent of maternal pre-pregnancy BMI and genetic predisposition to adiposity. Sci Rep, 12, 3135.
Schwarz SM. (2023). Obesity in children: Overview. Medscape. https://emedicine.medscape.com/article/985333-overview
Schweitzer L. (2024). The Engine 2 diet. https://www.webmd.com/diet/engine-2-diet
Seegert L. (2023). The cost of bariatric surgery in 2023. https://money.com/cost-of-bariatric-surgery/
Silva S. (2024). Is obesity a disease? What experts say. Healthline. https://www.healthline.com/health/is-obesity-a-disease#what-doctors-say
Skelton J. (2025). Prevention and management of childhood obesity in the primary care setting. UpToDate. https://www.uptodate.com/contents/management-of-childhood-obesity-in-the-primary-care-setting
Skelton J & Klish W. (2024a). Overview of the health consequences of obesity in children and adolescents. UpToDate. https://www.uptodate.com/contents/overview-of-the-health-consequences-of-obesity-in-children-and-adolescents
Skelton J & Klish W. (2024b). Comorbidities and complications of obesity in children and adolescents. UpToDate. https://www.uptodate.com/contents/comorbidities-and-complications-of-obesity-in-children-and-adolescents
Sloan M. (2024). What are the differences between popular low carb diets? https://www.health.harvard.edu/nutrition/what-are-the-differences-between-popular-low-carb-diets
Swami V. (2022). Why the body positivity movement risks turning toxic. https://theconversation.com/why-the-body-positivity-movement-risks-turning-toxic-189913
Sweis NJ. (2024). The economic burden of obesity in 2024: A cost analysis using the value of a statistical life. Critical Public Health, 34(1), 1–13. https://doi.org/10.1080/09581596.2024.2333407
Tampa General Hospital (TGH). (2025). Weight gain. https://www.tgh.org/institutes-and-services/conditions/weight-gain
Tarnowski A & Janssen S. (2021). Occupational therapy joining bariatric care teams: A web-based resource. https://commons.und.edu/cgi/viewcontent.cgi
Trout N. (2023). Reducing weight bias, stigma and discrimination. https://www.connecticutchildrens.org/advancing-kids/obesity-reducing-weight-bias-stigma-and-discrimination
U.S. Department of Agriculture (USDA). (2025). Food security in the U.S.—Key statistics & graphics. https://www.ers.usda.gov/topics/food-nutrition-assistance/food-security-in-the-us/key-statistics-graphics
University of California Irvine (UCI). (2024). Benefits of bariatric surgery. https://www.ucihealth.org/medical-services/bariatric-surgery/bariatric-surgery-benefits
Valicente V, Ching-Peng C, Pacheco K, et al. (2023). Ultraprocessed foods and obesity risk: A critical review of reported mechanisms. Advances in Nutrition, 14(4), 718–38.
Vandoni M, Marin L, Cavallo C, et al. (2024). Poor motor competence affects functional capacities and healthcare in children and adolescents with obesity. Sports, 12(2), 44. https://www.mdpi.com/2075-4663/12/2/44
Wainer A, Robinson L, et al. (2023). At the nexus of grocery access and transportation: Assessing barriers and preferences for alternative approaches to enhancing food access. Journal of Transport & Health, 33, 101712.
Weber. (2023). Stress and weight gain: The connection and how to manage it. https://www.medicalnewstoday.com/articles/stress-and-weight-gain
West M. (2022). What to know about the body positivity movement. https://www.medicalnewstoday.com/articles/body-positivity#what-is-body-positivity
Westbury S, Oyebode O, Rens T, & Barber T. (2023). Obesity stigma: Causes, consequences, and potential solutions. https://pmc.ncbi.nlm.nih.gov/articles/PMC9985585/
Williams J. (2023). Is a low-fat diet healthy? https://www.bbcgoodfood.com/health/special-diets/spotlight-low-fat-diets
Wojeck B. (2023). The connection between sleep, diabetes, and obesity. Yale Medicine. https://www.yalemedicine.org/news/sleep-diabetes-and-obesity
World Health organization (WHO). (2024). Obesity and overweight. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight
World Obesity. (2024). Prevalence of obesity. https://www.worldobesity.org/about/about-obesity/prevalence-of-obesity
World Obesity. (2022). Weight stigma. https://www.worldobesity.org/what-we-do/our-policy-priorities/weight-stigma
World Population Review. (2024). Obesity rates by country 2024. https://worldpopulationreview.com/country-rankings/obesity-rates-by-country
Wright GM, Huynh K, Schneider M, Gareau MG. (2024). Altering the gut microbiome for cognitive benefit. In N Hyland & C Stanton (Eds.), The gut-brain axis (2nd ed.), Academic Press. https://doi.org/10.1016/B978-0-323-99971-7.00011-4
Yang A. (2024). How sugar and fat affect your brain. National Geographic. https://www.nationalgeographic.com/magazine/article/how-sugar-and-fat-affect-your-brain
Yale Medicine. (2025). Bariatric surgery for weight loss. https://www.yalemedicine.org/conditions/bariatric-surgery-for-weight-loss
Yanovski S & Yanovski J. (2024). Approach to obesity treatment in primary care: A review. JAMA internal medicine, 184(7), 818–29. https://doi.org/10.1001/jamainternmed.2023.8526
Yearwood L & Masood W. (2024). Behavioral approaches to obesity treatment. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK570565/#:
Zaraska M. (2023). Foods can be literally addictive, new evidence suggests. Scientific American. https://www.scientificamerican.com/article/food-can-be-literally-addictive-new-evidence-suggests/
Zelman K. (2024a). Very low-calorie diets: What you need to know. WebMD. https://www.webmd.com/diet/low-calorie-diets
Zelman K. (2024b). The protein power diet. WebMD. https://www.webmd.com/diet/protein-power-what-it-is
Zhao S, Semeia L, Veit R, Luo S, et al. (2024). Exposure to gestational diabetes mellitus in utero impacts hippocampal functional connectivity in response to food cues in children. International Journal of Obesity, 48, 1728–34. https://doi.org/10.1038/s41366-024-01608-1
Customer Rating
4.9 / 784 ratings