A Look at Suicide: Prevention Training Program for Washington Healthcare Professionals (3 Hours)
Screening and Referral
Online Continuing Education Course

Course Description
3-hour mandatory suicide prevention training approved by the Washington State Department of Health. The following professions are required to take three hours of suicide prevention CE on suicide screening and referral: certified counselors and advisers, chemical dependence professionals, chiropractors, occupational therapists and assistants, physical therapists and assistants, and dental hygienists. This course meets the minimum requirements for pharmacists and dentists. Wild Iris Medical Education, Inc.'s training approval number is TRNG.TG.60722274-SUIC.
If you are in a crisis, call or text 988, call 911, or go to the nearest emergency room.
"Content was well organized, engaging, and concise. Very well done!" - Barbara, OT in Washington
"This was an excellent course. Thank you!" - Danielle, RN in Washington
"Great course! Amazing information that will help me in private practice as well as in my personal life with friends and family members dealing with suicidal thoughts. Thanks!" - Jacklyn, student in Washington
"Great course and definitely worth it!" - Jacob, chiropractor in Washington
This course fulfills the requirement for 3 hours of continuing education in suicide prevention, screening, and referral for OTs, PTs, and other healthcare professionals in Washington State. Wild Iris Medical Education, Inc.'s training approval number is TRNG.TG.60722274-SUIC.
Need 6 hours?









A Look at Suicide: Prevention Training Program for Washington Healthcare Professionals (3 Hours)
Screening and Referral
Copyright © 2026 Wild Iris Medical Education, Inc. All Rights Reserved.
LEARNING OUTCOME AND OBJECTIVES:
- Discuss the epidemiology and etiology of suicidal behavior.
- Summarize the risk and protective factors for suicide.
- Describe the process of assessment and determination of level of risk for suicide.
- Identify suicide prevention strategies.
- Discuss ethical dilemmas that arise in relation to suicide prevention and intervention efforts.
TABLE OF CONTENTS
UNDERSTANDING SUICIDE
Healthcare professionals play a critical role in the recognition, prevention, and treatment of suicidal behaviors, and the attitudes of these providers are paramount in how patients are treated. Historically, the stigma associated with suicide affects the attitudes of those who manage and treat these individuals.
Talk of suicide must always be taken seriously, recognizing that people with suicidal ideation are in physical or psychological pain and may have a treatable mental disorder. The vast majority of people who talk of suicide do not really want to die. They simply are in pain and want it to stop. Suicide is an attempt to solve this problem of intense pain when problem-solving skills are impaired in some manner, in particular by depression.
Many healthcare professionals express concern that they are ill prepared to deal effectively with a patient who has suicidal thoughts. By developing adequate knowledge and skills, these professionals can overcome feelings of inadequacy that may otherwise prevent them from effectively responding to the suicide clues a patient may be sending, thereby allowing them to carry out appropriate interventions. They can also develop a better understanding of this choice that ends all choices.
EPIDEMIOLOGY IN WASHINGTON STATE
Suicide is a leading cause of death, particularly among young people, veterans, middle-aged men, and American Indian and Alaska Natives (AI/AN). In 2023, approximately 1,300 Washington residents died by suicide, making it the eighth leading cause of death in the state. For nearly two decades, Washington’s suicide rate has consistently exceeded the national average. The economic and societal costs of suicide are also significant, estimated at over $12.8 billion annually in Washington alone (CDC, 2025c; WSDOH, 2025a).
By age: Suicide rates vary by age group. In 2022, suicide rates ranged from 1.75 per 100,000 among youth ages 10–14 years to 35.9 per 100,000 among people 85 years and older (WSDOH, 2025a).
By race/ethnicity: Suicide rates by race and ethnicity point to additional disparities. Suicide rates ranged from 8.6 per 100,000 among non-Hispanic Asian populations to 22.0 per 100,000 among non-Hispanic American Indian and Alaska Native (AI/AN) populations. In 2022, 76% of suicides occurred among non-Hispanic White populations (WSDOH, 2025a).
By sex: Suicide rates among females and males show large differences. In 2022, male age-adjusted suicide rates (23.6) were about four-fold higher than female rates (6.0) (WSDOH, 2025a).
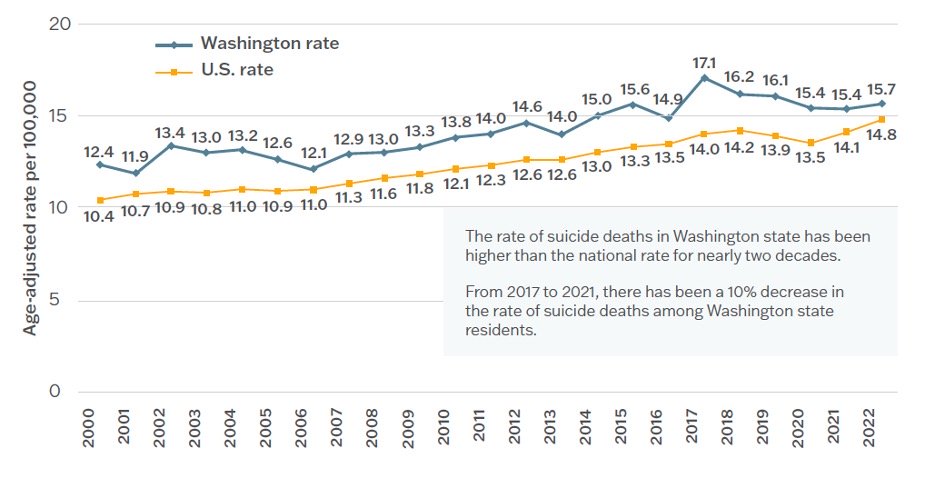
Age-adjusted suicide rates, 2000–2022, Washington and United States. (Source: WSDOH, 2025a.)
SUICIDE ETIOLOGY AND RISK AND PROTECTIVE FACTORS
Suicide etiology is complex and includes family history, genetics, epigenetics, neurobiology, medication use, and gender.
- Genetics: Four genes have been identified as heightening the risk of suicidal thoughts and actions (Avery, 2022).
- Epigenetics: The resulting impact of environmental influences on gene activity and expression has been associated with suicidal behavior (Dwivdei et al., 2025).
- Neurobiology: Inflammatory mediators have been found to play a critical role in the pathophysiology of suicide (Hu et al., 2025).
- Medications: Certain antidepressants and anticonvulsant drugs can increase the risk for suicide (Levin et al., 2026).
- Gender: The rate of suicide deaths in men is higher than in women; however, attempted suicide is more common among women than men.
Risk Factors for Suicidal Ideation
The risk factors for suicidal ideation can be subdivided into the categories of workplace stressors, home-life stressors, and individual risk factors.
Workplace stressors:
- Shift work / working hours
- Management issues
- Lateral violence (horizontal violence)
- Bullying
- Workplace conflict
- Inadequate preparation for role
Home life stressors:
- Financial stressors
- Relationship stressors
- Drug or alcohol use by self, family, or significant others
- Being the primary caregiver for children or parents
- Lack of an adequate support system
- Violent relationships
- Social relationships
- Family history of death by suicide
Individual risk factors:
- Previous suicide attempt(s)
- History of depression and other mental illnesses
- Chronic illness
- Substance use/abuse
- History of adverse childhood experiences (ACEs)
- Financial problems
- Legal/criminal problems
- Easy access to firearms and other means of death by suicide
- Feelings of hopelessness
(Baldini et al., 2025; CDC, 2024)
Suicide Protective Factors
Although there are many risk factors for suicide, there are also factors that protect people from making an attempt or dying by suicide. These protective factors are both personal and environmental.
Personal protective factors include:
- Values, attitudes, and norms that prohibit suicide, such as strong beliefs about the meaning and value of life
- Strong problem-solving skills
- Social skills, including conflict resolution and nonviolent ways of handling disputes
- Good health and access to mental and physical healthcare
- Strong connections to friends and family as well as supportive significant others
- Strong sense of cultural identity
- A healthy fear of risky behaviors and pain
- Optimism about the future and reasons for living
- Sobriety
- Medical compliance and a sense of the importance of health and wellness
- Good impulse control
- A strong sense of self-esteem or self-worth
- A sense of personal control or determination
- Strong coping skills and resiliency
- Being married or a parent
External/environmental protective factors include:
- Opportunities to participate in and contribute to school or community projects and activities
- Strong relationships, particularly with family members
- A reasonably safe and stable environment
- Availability of consistent and high-quality physical and behavioral healthcare
- Financial security
- Responsibilities and duties to others
- Cultural, religious, or moral objections to suicide
- Owning a pet
- Restricted access to lethal means
(AFSP, 2026c; CDC, 2024d)
Suicide Risk According to Age
Suicide occurs throughout the lifespan, affecting individuals in various age groups differently, and some have higher suicide rates than others.
CHILDREN AND ADOLESCENTS
Suicide is the second leading cause of death among U.S. children and adolescents ages 10–14 years and the third leading cause of death for those ages 15–24. In 2024, more than one third of visits to children’s hospitals’ emergency departments was from children and adolescents who exhibited suicidal ideation or behavior. Between 2016 and 2021, the number of suicide self-injury cases in patients ages 5–18 treated at children’s hospitals’ emergency departments increased by 168.6%. Not only are the numbers increasing in this population but so is the level of acuity (CHA, 2025).
Puberty may have a negative impact, especially for girls. Girls who mature early have been found to be more likely to have a lifetime history of disruptive behavior disorder and suicide attempts than their peers.
During adolescence, abstract and complex thinking begins to develop, and these youth become more capable of contemplating life circumstances, envisioning a hopeless future, generating suicide as a possible solution, and planning and executing a suicide attempt.
During adolescence, the prevalence of depression increases and becomes twice as high among girls than boys, which explains some differences in rates of suicide between boys and girls. As puberty progresses, most boys develop a positive self-image, but girls, particularly White girls, have a diminished sense of self-worth.
After puberty, the rate of suicide increases with increasing age. Potential reasons for this include an increased access to firearms and potentially lethal drugs; increased rates of psychiatric illness, substance abuse, and other comorbidities; or a history of aggressive, impulsive conduct with a tendency to act out emotions in damaging ways.
The risk of suicide among children and adolescents is increased due to:
- Family tensions
- Emotional and physical abuse
- Violence
- Lack of family connectivity
- Parental mental health problems
- Death of a loved one
- Family homelessness
- History of foster care and adoption
- Bullying
- Sexual orientation
- Substance abuse
(Kennebeck & Bonin, 2025; Sruthi, 2025)
SUICIDE IN ADOLESCENTS
Adolescents generally have a high suicide attempt rate, and those who are involved in certain subcultures have an even higher risk. For instance, there is an increased incidence of self-harm activities (such as cutting) in the “goth,” “emo,” and “punk” populations. Adolescents involved in repeated self-injury are up to eight times more likely to attempt suicide (Dean, 2025; Soreff, 2026).
It has been found that the rise in suicide and suicide attempts by adolescents correlates with the rise in electronic communication and social media. Increased digital media and smartphone use may influence mental health through several mechanisms, including the displacement of time spent in in-person social interactions, disruption of in-person social interactions, interference with sleep time and quality, cyberbullying, toxic online environments, and online information about self-harm (CDC, 2024a; Young et al., 2024).
YOUNG ADULTS
Young adults experience mental health challenges at historically high rates. Roughly 14% of adults aged 18–25 experience serious suicidal ideation every year. In the past decade, the suicide rate in young people ages 20–24 has increased 57%. One in 3 young adults has experienced a mental health issue in the past year, but only about 40% of adults who experience suicidal behaviors receive adequate mental healthcare (Bommersbach et al., 2022; Miron et al., 2019).
Asian American and LGBTQ+ young adults experience disproportionately high rates of suicide while American Indian and Alaska Native young people experience a rate of suicide 2.5 times higher than that of their peers.
Many young adults continue to deal with the consequences of the COVID-19 pandemic, which has resulted in high levels of depression, loneliness, anxiety, and trauma (Wiedemann et al., 2024).
The top reasons for suicide among young adults include:
- Depression, anxiety, and other mental health disorders
- History of substance abuse
- Exposure to violence, abuse, or other trauma, either chronic or acute
- Social isolation and loneliness
- Losing a family member through death or divorce
- Lack of educational opportunities
- Financial or job loss
- Limited affordable housing
- Conflict within relationships
- Starting or changing psychotropic medications
- Feeling stigmatized
- Lack of a support system
(The Jed Foundation, 2023)
MIDDLE-AGED ADULTS
Middle age (35–64 years) is a time of maximum risk, with suicide rates increasing in both middle-aged men and women, although men are much more likely than women to die by suicide. Middle-aged adults account for 8% of all suicide deaths in the United States, and suicide is the eighth leading cause of death for this age group (CDC, 2024b).
Middle age is a period characterized by high familial and social expectations, increased self-confidence, leadership, and community contribution, making midlife a time of well-being and peak functioning as well as a time of high stress. Well-being during this phase of life can vary considerably, from being confident and resilient when meeting changes and difficulties, to being nervous or overanxious in response to stressful events and conflicts.
Suicide rates for middle-aged women have increased more quickly compared to rates for men in recent years. Many of these women are in the “sandwich” generation, those who take care of their children as well as older parents. They are more likely to be very stressed as a result of the responsibilities they carry, increasing their risk for suicide.
In high-income countries across the globe, adults who experience financial stress are 74% more likely to die by suicide, and 87% of unemployed individuals are more likely to take their own lives than their peers who do not experience financial stress or job loss. Separation and divorce increase suicide risk by more than three times. People in this age group, especially men, consider work position, employment, and marital relationship as indicators of their social identity, and problems in these areas can be deeply distressing (Bateson, 2025; Sinyor et al., 2024; Tera, 2025).
DEATHS OF DESPAIR (DoD)
Over the past 20 years, there has been an increased mortality rate among middle-aged adults attributable to suicide, drug overdose, and alcohol abuse. These deaths are often referred to as “deaths of despair.” Factors related to these deaths include:
- Low socioeconomic position and education levels
- Working in jobs with high insecurity
- Unemployment
- Living in rural areas
- Rising medical costs
- Declining social cohesion
(Mejia et al., 2024)
OLDER ADULTS
Adults ages 65 and older comprise just 17% of the population but make up approximately 22% of suicides. Men 75 and older face the highest overall rate of suicide. Older adults tend to plan suicide more carefully and are also more likely to use more lethal methods. Among people who attempt suicide, 1 in 4 older adults will die by suicide, compared to 1 in 200 youths. Even if an older adult survives a suicide attempt, they are less likely to recover from the effects.
Loneliness has been found to top the list of reasons for suicide among this age group. Many of them are homebound, live on their own, and may lack the social connections needed to thrive. Other reasons may include:
- Grief over the loss of family members and friends and anxiety about their own death
- Loss of self-sufficiency and independence
- Greater likelihood of illnesses and chronic or debilitating diseases such as arthritis, cardiac problems, stroke, or diabetes, which compromise quality of life
- Loss of vision and hearing make it harder to do the things they’ve always enjoyed doing
- Cognitive impairment and dementia, which can affect a person’s decision-making abilities and increase impulsivity
- Financial stress, such as living on a fixed income or struggling to pay bills or afford food
- Clinical depression brought on by physical, emotional, and cognitive struggles
(NCOA, 2025)
Suicide Risk Among Specific Populations
Although suicide affects all groups of the population, the risk and protective factors for suicide may differ. The following summarizes risk and protective factors among specific populations.
PERSONS WITH DEMENTIA
Overall, people with dementia have no higher risk of dying by suicide than the general population, but the risk of suicide is significantly increased in people with a new diagnosis of dementia (within the first three months), those with a diagnosis of early onset dementia (younger than 65 years), and those with concurrent psychiatric illness. Risk of suicidal ideation increases after diagnosis and may be elevated at a moderate level of the disease. In people with dementia, younger age increases risk of death by suicide and being male increases risk of suicide behaviors.
Patients with early dementia may have greater cognition, giving them more insight into their disease and better enabling them to carry out a suicide plan. Severe dementia, however, could protect against suicide by decreasing a person’s capacity to implement a suicide plan. Also, impairment in cognition and personal activities of daily living are associated with greater risk of nursing home admission, which in itself is a risk factor for suicide (Desai et al., 2024).
CAREGIVERS
In 2025, 63 million U.S. adults provided ongoing care to adults or children with a medical condition or disability, representing almost one quarter of all adults in the country. These caregivers are usually spouses, older children, parents, and family friends. The average caregiver is 51 years old, and women account for 61% of caregivers. As a result of their significant social, economic, and personal contributions, caregivers experience high rates of physical and mental illness, social isolation, and financial distress. They are also at high risk for suicide.
There is an increased likelihood of developing suicide ideation among adults who are caregivers inside the home compared to those providing care outside the home. Additionally, those adults who are caring for parents (versus partners) inside the home had a greater likelihood of suicidal behaviors. Research indicates that the constant stress of providing activities of daily living inside the home is a risk factor for suicide. This is compounded in caregivers who provide activities of daily living support to dementia patients inside the home (Caregiving in the US, 2025; Van Orden, 2023).
MILITARY SERVICE PERSONNEL
Suicides among military service personnel have been steadily rising since 2000, and suicide is now the second leading cause of death among this group. Greater than 90% of military suicides are by male personnel who are most often younger than 35 years of age. Additionally, four times as many active-duty service members and veterans have died by suicide as died in battle since 9/11. Active-duty Army suicide rates are double that of other active member military services and two and a half times higher than the general population. In 2021, 17 or more veterans died by suicide each day. Service members are thought to have a decreased fear of death, high pain tolerance, and access to and familiarity with lethal weapons such as firearms, which increases their capability for suicide.
In a study asking a group of active-duty soldiers why they tried to kill themselves, all of the soldiers indicated a desire to end intense emotional distress. Other common reasons included the urge to end chronic sadness, a means of escaping people, or a way to express desperation. In addition, rates of mental health problems have risen 65% in the military since 2000, with nearly one million troops diagnosed with at least one mental health issue. Risk for suicide increases when military personnel experience both depression and posttraumatic stress together (ABCT, 2025; Smith, 2025).
Experiencing child abuse, being sexually victimized, and exhibiting suicidal behavior before enlistment are significant risk factors for service members and veterans, making them more vulnerable to suicidal behavior when coping with combat and multiple deployments. Military personnel reporting abuse as children have been found to be three to eight times more likely to report suicidal behavior. Sexual trauma of any type increases the risk for suicidal behavior. Men who have experienced sexual trauma are less likely than females to seek mental health care, which they may see as a threat to their masculinity. This is a strong predictor of suicide attempts in military personnel. Service members who attempted suicide before joining the military are six times more likely to attempt suicide post enlistment (APA, 2025).
Suicide among women in the military has increased at twice the rate of male service members. When compared to civilian women, those in the service are two to five times more likely to die by suicide. The primary reason is sexual trauma, particularly incidences of harassment and rape while stationed overseas, resulting from a pervading military culture that is antagonistic toward women in the military (Gorn, 2026).
There is strong evidence that among veterans who experienced combat trauma, the highest suicide risk has been observed in those who were wounded multiple times or were hospitalized as a result of being wounded.
Studies that looked specifically at combat-related posttraumatic stress disorder (PTSD) found that the most significant predictor of both suicide attempts and the preoccupation with thoughts of suicide is combat-related guilt about acts committed during times of war. Those with only some PTSD symptoms have been found to report hopelessness or suicidal ideation three times more often than those without PTSD (VA, 2025).
OCCUPATION-RELATED SUICIDE
Professions that are associated with high suicide rates include law enforcement, public safety officers, physicians, and firefighters. These professionals often work long, irregular hours; witness all types of injuries; and have exposure to guns, all of which places them at high risk for suicide. Many of these professionals use alcohol, and often the trigger is divorce. Physicians have a particularly high rate of divorce because of job-related stress and the reluctance to seek help (CDC, 2026; O’Rouke et al., 2023).
Among female nurses, the risk of death by suicide is nearly twice the risk observed in the general population. The COVID-19 pandemic has placed nurses at substantially higher risk for poorer mental health relative to other health professions (Norful, 2025).
SUICIDE SCREENING AND ASSESSMENT
Because a significant proportion of individuals who die by suicide have seen a health professional within a few days prior to their suicide attempt, suicide screening and assessment of risk for suicide are important steps to be taken in all healthcare settings.
Suicide prevention screening refers to a quick procedure in which a standardized instrument or tool is used to identify individuals who may be at risk for suicide and in need of assessment. It can be done independently or as part of a more comprehensive health or behavioral health screening.
Suicide assessment, as opposed to screening, refers to a more comprehensive evaluation done by a clinician to confirm a suspected suicide risk, to estimate imminent danger, and to decide on a course of treatment.
Suicide Screening
There is debate about the benefits of screening all patients (universal screening) for suicide risk factors and whether screening actually reduces suicide deaths. The general view, however, is that such screening should only be undertaken if there is a strong commitment to providing treatment and follow-up, since there is some evidence that screening improves outcomes when it is associated with close follow-up and treatment.
Instead of universal screening, some recommend that screening be done only for those presenting with known risk factors (selective or targeted screening). Despite this lack of uniform guidance, health systems are implementing suicide screening protocols, and screening tools are already widely used in primary care settings (O’Rourke et al., 2023).
U.S. PREVENTIVE SERVICES TASK FORCE RECOMMENDATIONS
The U.S. Preventive Services Task Force (USPSTF) recommends screening for major depressive disorder in the general adult population, including pregnant and postpartum persons, to reduce disparities in depression-associated morbidity. Screening should be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up. These recommendations parallel those of other organizations, such as the American College of Physicians, the American College of Preventative Medicine, the Institute for Clinical Systems Improvement, the American College of Obstetricians and Gynecologists, and the U.S. Department of Veteran Affairs (USPSTF, 2023).
JOINT COMMISSION RECOMMENDATIONS
The Joint Commission requires that all individuals from age 12 and above in all medical settings be screened for suicidal ideation using a validated tool. Patients who are screened and found positive for suicide risk on the screening tool should receive a brief suicide safety assessment conducted by a trained clinician to determine whether a more comprehensive mental health evaluation is required (TJC, 2026).
AMERICAN ACADEMY OF PEDIATRICS
The American Academy of Pediatrics’ age recommendations for suicide screening state:
- Youth ages 12 and over: Universal screening
- Youth ages 8–11: Screen when clinically indicated
- Youths under age 8: Screening not indicated; assess for suicidal thoughts/behaviors if warning signs are present
Young people require screening more frequently than adults, as adolescence and young adulthood are times of rapid developmental change and circumstances can shift frequently (AAP, 2023).
SCREENING TOOLS
The following are validated, evidence-based suicide risk screening tools.
- Beck Fast Scan: Seven questions that can help determine the intensity and severity of depression
- Suicide Risk Screen: 10-item questionnaire often used to screen for suicide in young people
- Patient Health Questionnaire (PHQ): Nine questions about self-harm, also used to identify patients at high risk of suicide
- SAFE-T: Can be used in an outpatient setting; offers insight into the extent and nature of suicidal thoughts and harmful behavior
- Columbia-Suicide Severity Rating Scale (C-SSRS): Available in multiple languages for prehospital use to assess for the presence of harmful behavior; also assesses for any known suicide attempts and suicide ideations and behaviors
- Ask (ASQ) Suicide Screening: Four brief questions to screen medical patients ages 8 years and above
- SBQ-R: A psychological, four-item questionnaire to identify risk factors for suicide in adolescents and adults
(CEBC, 2026; Columbia University, 2021; NIMH, 2026)
Recognizing Suicide Warning Signs
Besides screening for risk factors for suicide, it is important to be able to recognize statements, behaviors, and moods that indicate an individual may be at immediate risk for suicide.
Statements by a patient that constitute a suicide warning sign include language about:
- Killing oneself
- Feeling hopeless
- Having no reason to live
- Being a burden to others
- Feeling trapped
- Having unbearable pain
Behaviors that may signal risk—especially when related to a painful event, loss, or change—include:
- Increased use of alcohol or drugs
- Searching for a method to end their life, for example, online search
- Withdrawing from activities
- Risky behaviors
- Isolating from family and friends
- Sleeping too much or too little
- Visiting or calling people to say goodbye
- Giving away prized possessions
- Aggression
- Fatigue
- Writing a will and making final arrangements
People considering suicide often display one or more of the following moods:
- Depression
- Anxiety
- Loss of interest
- Irritability
- Humiliation/shame
- Agitation/anger
- Relief / sudden improvement
(AFSP, 2026c)
Suicide Risk Assessment
The purpose of a suicide risk assessment is to determine a patient’s risk and protective factors with a focus on identification of targets for intervention. The most effective assessment begins with the establishment of a therapeutic relationship with the patient.
ESTABLISHING RAPPORT
The initial contact with a person with suicidal thoughts may occur in many different settings—home, telephone, inpatient unit, outpatient clinic, practitioner’s office, rehabilitation unit, long-term care facility, or hospital emergency department. Being skilled at establishing rapport quickly is essential for all clinicians. It is imperative that the person be given privacy, be shown courtesy and respect, and be made aware that the clinician wants to understand what has happened or is happening to them.
CULTURAL PERSPECTIVES ON SUICIDE
Clinicians should be aware of the cultural perspectives on suicide to build rapport with patients. For example, in some Eastern cultures suicide is seen as noble or honorable if done for political or social causes. In Japan, suicide is viewed as “morally responsible” when performed as a ritual, although in recent years Japanese students have advocated for national suicide prevention strategies. In Western cultures, suicide is largely stigmatized and viewed as shameful and cowardly. In many African cultures, suicide is taboo due to its perceived association with evil spirits and inherent curses. Indigenous cultures, particularly in North America, face high suicide rates due to generational trauma, loss of cultural identity, and issues related to poverty. Suicide is regarded as a symptom of the culture’s broader collective trauma (Jobes, 2026).
Basic Attending Skills
Basic attending and listening skills are valuable in establishing rapport and a therapeutic alliance in order to obtain information, set the foundation for the treatment plan, and assist in determining interventions. These skills range from nondirective listening behaviors to more active and complex ones.
Positive attending behaviors are nonverbal and include:
- Eye contact. Maintaining eye contact communicates care and understanding and can show empathy and an interest in the person’s situation. Cultures vary in what is considered appropriate. Asian and Native Americans, for example, may view eye contact as aggressive.
- Body language. Usually leaning slightly toward the patient and maintaining a relaxed but attentive posture is effective. This may also include mirroring, which involves matching the patient’s facial expression and body posture.
- Vocal qualities. These include tone and inflections of the interviewer’s voice. Tonal quality may move toward “pacing,” which is matching the patient’s vocal qualities. Vocal qualities can be used to lead the patient.
- Verbal tracking. This involves using words to demonstrate that the interviewer has accurately followed what the patient is saying, such as restating or summarizing what the patient has said.
Negative attending behaviors include:
- Overuse of positive attending behaviors, which can become negative or annoying
- Turning away from the patient
- Making infrequent eye contact
- Leaning back from the waist up
- Crossing the legs away from the patient
- Folding the arms across the chest
(Grieve, 2023)
Listening Skills and Action Responses
Effective interviewing also requires nondirective and directive listening as well as directive action responses.
Nondirective listening responses include those described below.
- Silence is a skill requiring practice to be comfortable with. It is very nondirective, and if used appropriately, it can be very comforting for the patient.
- Nondirective questioning includes asking for clarification, more facts, and details and is best done by using open-ended questions.
- Paraphrasing, or reflection, is a verbal tracking skill that involves restating or rewording what the patient has said. There are three types of paraphrasing that can be utilized:
- Simple paraphrasing gives direction but involves rephrasing the core meaning of what the patient has said.
- Sensory-based paraphrasing involves the interviewer using the patient’s sensory words in the paraphrase (visual, auditory, kinesthetic, etc.).
- Metaphorical paraphrasing involves making an analogy or metaphor to summarize the patient’s core message.
- Intentionally directive paraphrasing is solution focused and attempts to lead the patient toward more positive interpretations of reality.
- Empathizing is used to show that the listener identifies with the patient’s information and allows the patient the right to their feelings.
- Supporting includes agreement, offers to help, reassurance, and focusing on the here and now.
- Analyzing is helpful in gaining different alternatives and perspectives by offering an interpretation of the patient’s message, making sure the person will be receptive.
- Summarization is an informal summary of what the patient has said. It should be interactive, encouraging, and supportive and include positives or strengths that may help the patient cope.
(Sommers-Flanagan, 2024; Wrench et al., 2026)
Directive listening skills include those described below.
- Validating feelings involves acknowledgement and approval of the patient’s emotional state. It can help patients accept their feelings as normal or natural and can enhance rapport.
- Interpretive reflection of feeling, also referred to as advanced empathy, goes beyond surface feelings or emotions to uncover deeper, underlying feelings, which can bring about strong emotional insights or defensiveness.
- Interpretation, also known as reframing, is a classic psychoanalytic technique that can produce patient insight or a solution-focused way to help patients view their problems from a new and different perspective.
- Confrontation involves pointing out perceptual inaccuracies or inconsistencies to help the patient see reality more clearly. It works best when excellent rapport has been established, and it can be either gentle or harsh.
(Sommers-Flanagan, 2022)
When attempting to elicit information from persons who are contemplating suicide, it should be remembered that challenging or direct questions, which could be interpreted as critical, will rarely be of benefit. The individual with suicidal thoughts should be encouraged and given the opportunity to express thoughts and feelings and be allowed to discharge pent-up and repressed emotions. Asking open-ended questions encourages the person to elaborate on their answers, which can provide important context on their level of risk, access to means, and presence of intent (Aamar, 2025).
| Person’s Statement | Appropriate Responses |
|---|---|
| Everyone will be better off without me. |
|
| I just can’t bear it anymore. |
|
| I just want to go to sleep and not deal with it again. |
|
| I want it to be over. |
|
| I won’t be a problem much longer. |
|
| Things will never work out. |
|
| It is all so meaningless. |
|
ASSESSING SUICIDAL INTENT
Once it is determined that suicidal ideations are present, the next step is to determine whether the patient’s intent is active (thoughts of taking action) or passive (wish or hope to die). The patient should be asked if the thoughts are new and if there are changes in the frequency or intensity of chronic thoughts. It is also important to inquire about the patient’s ability to control these thoughts.
The next step is to determine if the patient has developed a suicide plan and their degree of intent. This includes asking whether or not they have made any preparations and what they are. It is also important to determine whether the patient has a history of impulsive behaviors or substance use that may increase impulsivity and whether they have a past history of suicidal ideation and behavior.
In addition, the clinical interview includes observing whether the patient is disconnected, disengaged, or shows a lack of rapport, as these signs are associated with an increased risk of suicide (Schreiber & Culpepper, 2025).
Suicide Risk Assessment Tools
Although various suicide risk assessment tools are available, experts have repeatedly come to the conclusion that there is not any one tool that can predict who will die by suicide to any useful degree.
There are many tools available to assist healthcare professionals in determining suicidal intent. These assessment tools are used to assess a person’s intent to carry through. They are often used when positive results have been obtained with one of the screening tools mentioned above. The following are validated/evidence-based suicide risk assessment tools.
- Ask Suicide Screening Questions (ASQ) Toolkit is a four-item suicide screening tool designed to be used for people of all ages in emergency departments, inpatient units, and primary care facilities.
- Columbia-Suicide Severity Rating Scale (C-SSRS), Risk Assessment version. The risk assessment version of this tool provides a checklist of protective and risk factors for suicide and is used along with the C-SSRS screening tool. It is appropriate in all settings for all ages and for special populations in different settings. The tool features a clinician-administered initial evaluation form, a “since last visit” version, and a self-report form. The Columbia protocol questions have also been incorporated into the SAMHSA SAFE-T model with recommended triage categories.
- Beck Scale for Suicide Ideation (BSI). This 21-item self-report instrument can be used in inpatient and outpatient settings for detecting and measuring the current intensity of the patient’s specific attitude, behaviors, and plans to die by suicide during the preceding week. It assesses the wish to die, desire to make an active or passive suicide attempt, duration and frequency of ideation, sense of control over making an attempt, number of deterrents, and the amount of actual preparation for the contemplated attempt.
(TJC, 2026)
Clinical Interview
The clinical interview is the gold standard for suicide assessment and intervention. Topics covered during this interview include suicidal ideation, plans, self-control, intent, and safety planning.
Following are three effective approaches to asking about suicide.
- Use a normalizing tone. About 60% of people who died by suicide denied suicidal ideation when asked by a healthcare provider, indicating the presence of psychological and interpersonal barriers to disclosure. It is helpful to use a statement that normalizes suicide ideation, such as: “I asked you this question because almost all people at one time or another have thoughts about suicide.”
- Use gentle assumption. To make it easier for patients to disclose suicidal ideation, the interviewer assumes that certain thoughts and behaviors are already occurring in the person and gently structures questions accordingly. So, instead of asking if the person has been thinking about suicide, ask “When was the last time you had thoughts about suicide?”
- Assess the person’s mood. An exploration of mood states might include asking permission to discuss mood and then asking patients to rate their mood using a 0–10 scale. This is followed by questions that refer to the worst or lowest mood rating the person has ever had as well as what was happening at those times that made them feel so down. In order to end with a positive note, the patient is asked about the best mood rating they’ve ever had.
Explore suicidal ideation. When the patient discloses the presence of suicidal ideation, collaboratively explore the frequency, triggers, duration, and intensity of the suicidal thoughts. During this process, it is important to show curiosity, empathy, and interest instead of judgment. If the patient denies suicidal thoughts and the denial appears to be genuine, acknowledge and accept the denial, but if the denial seems forced or is combined with symptoms of depression or other risk factors, acknowledge and accept the denial but return to the topic later.
Explore suicide plans. Once rapport is established and the patient has talked about suicidal ideation, it is important to explore suicide plans. If patients admit to a plan, further exploration is crucial. Evaluation includes assessing the specificity of the plan, its lethality, availability of the means, and proximity of social support (i.e., availability of individuals who might intervene and rescue the patient) (see “Assessing the Plan, Lethality, and Risk” below).
Assess self-control. This requires asking directly about self-control and observing for agitation, arousal, or impulsivity. Arousal and agitation adversely affect self-control and are the inner push that drives persons toward suicidal acts (Sommers-Flanagan, 2022).
STEPS TO TAKE WHEN A PATIENT REFUSES ASSESSMENT
- Obtain information from other sources, such as:
- Collateral reports from staff
- Patient’s past medical records
- Past suicide attempts
- Past nonsuicidal self-injury
- Past episodes of suicidal thinking
- Mental status assessment
- For patients who are competent and refuse services, document efforts made to gain cooperation.
- Document an explanation of the limitations of assessment and how level of risk was determined.
(Werne, 2024)
ASSESSING THE PLAN, LETHALITY, AND RISK
The evaluation of a suicide plan is extremely important in order to determine the degree of suicidal risk. When assessing the lethality of a plan, it is important to learn all the details about the plan, the method chosen, and the availability of means. People with definite plans for a time, place, and means are at high risk for suicide. Someone who is considering suicide without making a plan is at lower risk.
Suicide deaths are more likely to occur when persons use highly damaging, fast-acting, and irreversible methods—such as jumping from heights or shooting—and do so when rescue is fruitless.
IMPULSIVITY AND SUICIDE
Some suicides are carefully planned and deliberate, while others appear to have been impulsively decided upon, involving little or no planning. Impulsiveness is thought to play an instrumental role in suicide because of the presumption that suicidal behaviors are carried out via rash decisions with little consideration for the consequences. A study of survivors of nearly lethal suicide attempts found that 1 in 4 individuals deliberated for less than five minutes. Another study found that 47% reported deliberating an hour or less (HSPH, 2023).
A recent study has found an altered pattern of ventromedial prefrontal cortex and frontoparietal connectivity in impulsive people who exhibit suicidal behavior, as well as reduced ventromedial prefrontal cortex value signals. This altered connectivity has been found to be disrupted in people who attempted suicide and is believed to underlie disrupted choice processes in a suicidal crisis (Wislowska-Stanek et al., 2021).
Methods of Suicide and Lethality
The desire for a painless method of suicide often leads individuals to choose a method that tends to be less lethal. This results in attempted suicides that do not end in death. For every 25 attempts, there is one death. For drug overdoses, the ratio is around 40 to 1.
The most common fatal methods of suicide are:
- Firearms: 52%
- Suffocation/hanging: 23%
- Poisoning/overdose: 18%
- Jumping: 2%
- Cutting: 2%
- Other: 4%
The most nonfatal methods of self-harm treated in the emergency department are poisoning/overdose (64%), cutting (19%), and firearms (1%) (HSPH, 2023).
It is of utmost importance for clinicians to recognize that these methods, as well as other highly lethal suicide methods, are widely accessible and must be considered when determining the disposition of someone who has suicidal ideations.
Factors that influence the lethality of a chosen method include:
- Intrinsic deadliness. A gun is intrinsically more lethal than a bottle of pills.
- Ease of use. If a method requires technical knowledge, for example, it is less accessible than one that does not.
- Accessibility. Given the brief duration of some suicidal crises, a gun in the cabinet in the hall is a greater risk than a very high building 10 miles away.
- Ability to abort mid-attempt. More people start and stop mid-attempt than carry through. It is easier to interrupt a hanging or to call 911 after overdosing than to stop a method such as jumping off a bridge or using a gun.
- Acceptability to the individual. The method must be one that does not cause too much pain or suffering. For example, fire is readily accessible, but it is a method seldom used in the United States.
(HSPH, 2023)
Level of Risk
A clinical judgment that is based on all the information obtained during assessment should help to assign a level of risk for suicide and determine the setting of care.
Patients who are low risk of suicide:
- Are experiencing recent suicidal ideation or thoughts
- Have no specific current suicide plan
- Have no clear intent to act
- Have not planned or rehearsed a suicide act
- Have identifiable and multiple protective factors
- Have limited risk factors
- Have no history of suicidal behaviors
- Have evidence of self-control
- Have supportive family members or significant others
- Have a high degree of ambivalence
Most people with suicidal ideation do not necessarily want to die; they just do not want to continue living in an intolerable situation or state of mind. This ambivalence is one of the most important tools for working with such persons. Almost everyone with suicidal thoughts is ambivalent about dying, leaning toward suicide at one moment in time and then leaning toward living the next. The healthcare professional can use this ambivalence to help focus the person on the reasons why they should live.
Patients who are at moderate risk:
- Have current suicide ideation
- Have no clear plan for suicide
- Have had no preparatory behavioral or rehearsal of act
- Have limited or no intention to act
- Have limited identifiable protective factors
- Are able to control the impulse
- Have the ability to maintain safety, independent of external support
- Have no recent suicidal behavior
- Have supportive family or significant others
- Have a high degree of ambivalence
Patients who are at high/severe/imminent risk:
- Have strong, persistent suicidal ideation
- Have strong intention to plan or act
- Have a specific suicide plan
- Have access to lethal means
- Have minimal protective factors
- Have impaired judgment
- Have poor self-control either at baseline or due to substance use
- Have inability to maintain safety, independent of external support
- Have a poor social support network
- Have severe psychiatric symptoms or an acute precipitating event
- Have a history of prior suicide attempt
(VA, 2024)
PREDICTING SUICIDE BY RISK LEVEL
There has been no improvement in the accuracy of predicting suicides in the past 40 years.
- 95% of “high-risk” patients will not die by suicide.
- 50% of suicides are from “low-risk” patients.
- 50% of individuals who die by suicide have no prior history of suicide attempts.
(PsychDB, 2025)
Differentiating between Non-Suicidal Self-Injury and Suicide Attempt
Healthcare professionals are increasingly confronted with another problem related to suicide attempts called non-suicidal self-injury (NSSI). DSM-5 defines NSSI as the “deliberate, self-inflicted destruction of body tissue without suicidal intent and for purposes not socially sanctioned” (APA, 2013).
Self-harm is a sign of emotional distress, and adolescents are at the highest risk, with approximately 15% of teenagers and 17%–35% of college students having been found to inflict self-harm injury. Both males and females have similar rates of NSSI.
Studies have found the following reasons given for engaging in self-harm behavior:
- To feel a sense of control over the body or life situations
- To punish oneself for perceived faults
- To reduce negative emotions
- To feel “something” instead of numbness or emptiness
- To avoid certain social situations
- To receive social support
The greatest difference between suicide and self-harm is intent. Suicide is a method that can end pain, but self-harm is an act to enhance coping with feelings and stressors. Some individuals find that pain from self-injury is reassuring when they are feeling numb or disconnected from the world around them. NSSI, however, can increase the risk of suicide because of the emotional problems that trigger self-injury and the pattern of damaging the body in times of distress.
It is important to keep in mind that the act of self-harm induces pain receptors that trigger the brain to feel an adrenaline “rush.” This can readily become addictive and highly dangerous (Discovery Mood & Anxiety Program, 2025; Mayo Clinic, 2024).
ASSESSMENT OF NSSI PATIENTS
Assessment of the patient who presents with non-suicidal self-injurious behavior includes:
- Determining what type of injury and how many types of injuries the patient has inflicted
- Determining how often non-suicidal self-injury occurs and how long it has been occurring
- Determining the function of NSSI for the patient
- Assessing for coexisting psychiatric disorders
- Estimating the risk of suicide attempt
- Determining how willing the patient is to participate in treatment
The most common examples of NSSI include cutting or stabbing the skin with a sharp object and burning the skin. Patients often injure themselves repeatedly in a single session, creating multiple lesions in the same location, typically in areas that are easily hidden but accessible, such as the forearms, chest, abdomen, or front of the thighs. The behavior is often repeated, resulting in extensive patterns of scarring (Moutier, 2026).
Signs of NSSI that may be found during the physical examination include:
- Scars, often in patterns
- Fresh cuts, scratches, bruises, bite marks, or other wounds
- Wearing long sleeves or long pants to hide self-injury, even in hot weather
- Frequent reports of accidental injury
(Mayo Clinic, 2024)
Once signs of NSSI are identified, an assessment tool can be used to aid in diagnosing NSSI and differentiating patients who are at increased risk of suicide. These may be either self-administered or clinician administered. Examples include:
- Self-Harm Behavior Questionnaire (SHBQ)
- Suicidal Behaviors Questionnaire (SBQ)
- Self-Injurious Thoughts and Behaviors Interview (SITBI)
- Suicide Attempt Self-Injury (SASSI)
- The Ottawa Self-Injury Inventory (OSI)
- The Child Behavior Checklist (CBCL)
(Wikiversity, 2023)
Documentation of Suicide Risk Assessment
Good documentation is basic to clinical practice. Accurate, sufficiently detailed, and concise records of a patient’s treatment allow for quality care and communication among providers. The best records reflect awareness of risk and the process of professional judgement that recognized it, took steps to reduce it, and balanced it with patient needs. Documentation to be added to the patient record includes:
- Reason for suicide assessment
- Review of past available records
- Evaluation of warning signs and risk and protective factors
- Initial and ongoing suicide risk assessment
- Access to lethal means and mitigation
- Consultations with colleagues
- Referrals to behavioral health
- Rationale and follow-up for treatment options
- Safety planning and discharge coordination
- Plans for follow-up
(Chiles et al., 2024)
MODELS OF CARE FOR PATIENTS AT RISK FOR SUICIDE
A model of care is a set of interventions that can be consistently carried out in various settings to ensure that people get the right care at the right time, by the right provider or team, and in the right place. Newer models of care for management of patients at risk for suicide include:
- Crisis support and follow-up (e.g., center hotline)
- Brief intervention and follow-up
- Suicide-specific outpatient management
- Emergency respite care
- Tele–mental health
- Inpatient psychiatric hospitalization, with suicide-specific treatment
(EDC, 2026)
Crisis Support and Follow-Up
Crisis support and follow-up can include mobile crisis teams, walk-in crisis clinics, hospital-based psychiatric emergency services, peer-based crisis services, and other programs designed to provide assessment, crisis stabilization, and referral to an appropriate level of ongoing care. Crisis centers can also serve as a connection to the patient between outpatient visits and are helpful for patients with barriers to accessing outpatient mental health services. Crisis services also include care coordination. Mobile crisis teams provide care in the community at the location of the person who has suicidal thoughts (EDC, 2026).
Brief Intervention and Follow-Up
Brief interventions range from a single, in-person session to a computer-administered intervention in a primary care office to an online screening and feedback intervention that can be done on a personal electronic device. Brief interventions can be an immediate intervention and also can be used in conjunction with any other level of care. Safety planning is recommended for those who refuse outpatient care. Outreach and follow-up are provided through phone calls, letters, and texts (EDC, 2026).
Suicide-Specific Outpatient Management
Suicide-specific outpatient management involves several sessions that may include dialectical behavior therapy, cognitive therapy for suicide prevention (CT-SP), and collaborative assessment and management of suicide (CAMS). It is critical that outpatient mental health providers monitor patients between appointments and follow up when patients miss appointments (EDC, 2026).
Emergency Respite Care
Emergency respite care is an alternative to inpatient or emergency department services for a person in a suicidal crisis when the person is not in immediate danger. Respite centers are usually located in residential facilities designed to be more like a home than a hospital. These facilities may include staff members who are peers who have lived experience of suicide. Respite care is increasingly being utilized as an intervention and may include help with establishing continuity of care and provision of longer-term support resources, as well as support by text, phone, or online following a stay (EDC, 2026).
Tele–Mental Health
Tele–mental health involves electronic communication to provide clinical mental health services from a distance. Healthcare organizations can use these services to provide emergency assessments and treatment, especially for those patients located in remote geographic regions and for organizations with limited access to mental health resources (EDC, 2026).
Hospitalization
Inpatient hospitalization is the most restrictive option for addressing suicide risk. Research has found that patients may be at higher risk immediately after discharge from inpatient care. The reasons why this may happen are not known; however, experts have questions as to whether there is something about the experience of hospitalization itself that may be harmful. Involuntary hospitalization has been found to be associated with increased risk of suicide both during the hospitalization and afterward. It is therefore recommended that hospitalization be carefully weighed against other options (EDC, 2026).
SUICIDE PREVENTION STRATEGIES
Effective suicide prevention is a comprehensive undertaking requiring the combined efforts of every healthcare provider and addressing different aspects of the problem. A model of this comprehensive approach includes:
- Identifying and assisting persons at risk. This may include suicide screening, teaching the warning signs of suicide, and providing gatekeeper training (see below).
- Ensuring access to effective mental health and suicide care and treatment in a timely manner and coordinating systems of care by reducing financial, cultural, and logistical barriers to care.
- Supporting safe transitions of care by formal referral protocols, interagency agreements, cross-training, follow-up contacts, rapid referrals, and patient and family education.
- Responding effectively to persons in crisis by ensuring crisis services are available that provide evaluation, stabilization, and referrals to ongoing care.
- Providing for immediate and long-term postvention to help respond effectively and compassionately to a suicide death, including intermediate and long-term supports for people bereaved by suicide (see “Postvention for Suicide Survivors” below).
- Reducing access to lethal means by educating families of those in crisis about safe storage of medications and firearms, distributing gun safety locks, changing medication packaging, and installing barriers on bridges.
- Enhancing life skills and resilience to prepare people to safely deal with challenges such as economic stress, divorce, physical illness, and aging. Skill training, mobile apps, and self-help materials can be considered.
- Promoting social connectedness and support to help protect people from suicide despite their risk factors. This can be accomplished through social programs and other activities that reduce isolation, promote a sense of belonging, and foster emotionally supportive relationships.
(SPRC, 2025a, 2025c)
Public Health Suicide Prevention Strategies
The Centers for Disease Control and Prevention “Suicide Prevention Resource for Action” details the strategies based on the best available evidence to help states and communities prevent suicide.
- Strengthen economic supports
- Strengthen household financial security
- Stabilize housing
- Create protective environments
- Reduce access to lethal means among persons at risk of suicide (see below)
- Create healthy organizational policies and culture
- Reduce substance use through community-based policies and practices
- Improve access and delivery of suicide care
- Cover mental health conditions in health insurance policies
- Increase provider availability in underserved areas
- Provide rapid and remote access to help
- Create safer suicide care through systems change
- Promote healthy connections
- Promote healthy peer norms
- Engage community members in shared activities
- Teach coping and problem-solving skills
- Support social emotional learning programs
- Teach parenting skills to improve family relationships
- Support resilience through education programs
- Identify and support people at risk
- Train gatekeepers (see below)
- Respond to crises
- Plan for safety and follow-up after an attempt
- Provide therapeutic approaches
- Lessen harms and prevent future risk
- Intervene after suicide (postvention) (see below)
- Report and message about suicide safely
(CDC, 2024c)
GATEKEEPER TRAINING PROGRAMS
Gatekeeper training (GKT) is one of the most widely used suicide prevention strategies. It involves training people who are not necessarily clinicians to be able to identify individuals experiencing suicidality and refer them to appropriate services. GTK improves people’s knowledge, skills, and confidence in helping those who experience suicidal ideation and enhances positive beliefs about the efficacy of suicide prevention (Hawgood et al., 2022).
One example of gatekeeper training, QPR, involves three steps—Questions, Persuade, and Refer—that can be learned in as little as two hours (Purdue University, 2025).
VETERANS HEALTH ADMINISTRATION PREVENTION FRAMEWORK
Within the Department of Veterans Affairs (VA), the Veterans Health Administration’s approach to suicide prevention is based on a public health framework that focuses on intervention within populations rather than a clinical approach that intervenes with individuals.
This public health perspective considers questions such as:
- Where does the problem begin?
- How can we prevent it from occurring in the first place?
The VA follows this systematic approach:
- Define the problem by collecting data to determine the who, what, where, when, and how of suicide deaths.
- Identify and explore risk and protective factors using scientific research methods. Develop and test prevention strategies.
- Assure widespread adoption of strategies shown to be successful.
(VA, 2018)
Under the Veterans Comprehensive Prevention, Access to Care, and Treatment (COMPACT) Act of 2020, veterans in suicidal crisis can receive free emergency healthcare at any VA or non-VA healthcare facility (VA, 2023).
Resources available for veterans and their families include:
- Suicide Prevention Coordinator, available at each VA medical center, who provides veterans with counseling and other services; as appropriate, callers to the Veterans Crisis Line are referred to their local coordinator
- Coaching Into Care, a national telephone service to educate, support, and empower family members and friends seeking care or services for a veteran (call 888-823-7458)
- Veterans Crisis Line (call 988 or text 838255)
- Suicide Safety Plan template
- inTransition, a free, confidential program offering coaching and specialized assistance over the phone for active-duty service members, Guard and Reserve members, and veterans who need access to mental health care
- Make the Connection, an online resource that connects veterans, family members, friends, and other supports with information and solutions to issues affecting their lives
- Vet Centers’ readjustment counseling services
(VA, 2018)
Washington State Suicide Prevention Initiatives
Washington State’s first suicide prevention plan was written in 1995 by the Department of Health (DOH) and the University of Washington’s School of Nursing to address youth suicide prevention. That plan was revised in 2009 and again in 2014. Washington’s first comprehensive plan for suicide prevention for people of all ages was released in 2016, and the latest plan was released in 2025 and will extend through 2034.
The Washington Suicide Prevention Plan (WSDOH, 2025b) is guided by five core principles:
- Centering lived experience
- Partnerships and collaborations
- Safe and effective messaging and reporting
- Evidence-based prevention
- Culturally informed approaches
Washington’s plan is further organized into four strategic directions, each with specific goals and objectives. These play an important part in a comprehensive approach to suicide prevention and align closely with the 2024 National Strategy for Suicide Prevention:
- Healthy and connected individuals, families, and communities
- Multisector suicide prevention
- Treatment and crisis services
- Data collection, quality improvement, and research
Forefront Suicide Prevention is a Center of Excellence at the University of Washington focused on reducing suicide. Forefront has trained more than 30,000 health and school professionals and community members statewide in suicide awareness, intervention, and response skills. Efforts include:
- LEARN Suicide Prevention, a training in suicide awareness, intervention, and response skills
- Forefront Community Organizers, a volunteer support network for those who have attempted suicide and those who have lost a loved one to suicide
- Forefront Cares peer-to-peer mentoring program for newly bereaved individuals
- Safer Homes, Suicide Aware, a campaign that focuses on safe storage of medications and firearms (see box below)
Reducing Access to Lethal Means
When a person is at risk for suicide, actions are required to removal lethal means. There are many actions that can be taken by families, organizations, healthcare providers, and policymakers to reduce access to lethal means of self-harm. Examples include reducing access to medications and safe storage of firearms.
Responsible firearm storage involves keeping them locked and preferably unloaded and separating firearms and ammunition when not in use. Secure storage options include either storing firearms away from home or locked at home in a secure gun safe, gun cabinet, or lockbox. In addition, unloaded firearms can be secured with a gun-locking device or can be disassembled with parts securely locked in separate locations.
When considering temporary gun storage with friends or relatives, under federal law, a person should not ask someone to store their firearm if that person is prohibited from possessing a firearm.
Reducing means of suffocation includes taking measures to reduce suicide by hanging. About 10% of suicides by hanging occur in the controlled environments of hospitals, prisons, and police custody. The remainder occur in the community, where ligatures and ligature points are all widely available. Healthcare systems can reduce suicide by hanging by installing collapsible shower heads, light fixtures, door knobs, and providing bedding that is resistant to tearing.
Safety measures available for individual storage and disposal of prescription and nonprescription drugs include drug lockboxes, drug buyback programs, and confidential drug return programs. Many states, including Washington, also have similar online tools to identify local collection sites and resources (NAASP, 2020). (See also “Resources” at the end of this course.)
Collaborating with members of the community to increase public safety can include:
- Instituting lethal means counseling policies in health and behavioral healthcare settings and training healthcare providers in those settings
- Passing policies that exempt at-risk patients from 90-day refill policies
- Working with gun retailers and gun owner groups on suicide prevention efforts
- Distributing free or low-cost gun locks or gun safes
- Ensuring that bridges and high buildings have protective barriers
(SPRC, 2025c)
WASHINGTON’S SAFER HOMES, SUICIDE AWARE
In Washington, about 75% of gun deaths are suicides, and medication overdoses are the most frequent type of suicide attempt. Safer Homes, Suicide Aware, a program led by the University of Washington’s Forefront Suicide Prevention center, focuses on access to lethal means, particularly firearms and medications. The program targets men ages 35–64 and veterans, groups that are statistically more likely to use firearms in suicide attempts. Efforts include:
- Partnering with firearms retailers, medical providers, pharmacy professionals, and veteran-serving organizations to make sure each group understands its crucial role in preventing suicides
- Engaging directly with community members at public events ranging from gun shows to National Night Out gatherings
- Offering free locks in exchange for participation in a survey about secure storage practices and suicide risk awareness
(WSDOH, 2025b)
Postvention for Suicide Survivors
All settings should incorporate postvention as a component of a comprehensive approach to suicide prevention. Postvention is a term often used in the suicide prevention field. It is an organized response in the aftermath of a suicide to accomplish any one or more of the following:
- To facilitate the healing of individuals from grief and stress of suicide loss
- To alleviate negative effects of exposure to suicide
- To prevent suicide among people who are at high risk after exposure to another’s suicide
Postvention ensures that individuals and families who have experienced a suicide or suicide attempt are offered support. Postvention activities are intended to normalize anger, minimize self-blame, help survivors find meaning in the victim’s life, and be sensitive to cultural differences regarding suicide.
Key principles for creating a comprehensive postvention effort include:
- Planning ahead to address individual and community needs
- Providing immediate and long-term support
- Tailoring responses and services to the unique needs of suicide-loss survivors
- Involving survivors of suicide loss in planning and implementing postvention efforts
All suicide prevention efforts should include a comprehensive postvention component that reduces risk and promotes healing for the immediate family and reaches out into the community to support the broader group of loss survivors, including friends, coworkers, first responders, treatment providers, and others exposed to the death (SPRC, 2025b).
INSURANCE COVERAGE FOLLOWING SUICIDE OR ATTEMPTED SUICIDE
There are federal protections to ensure that most health insurance plans will pay for medical care resulting from a suicide attempt. There are, however, many forms of health insurance, and some plans may expose people to substantial uncovered costs after an attempted suicide (Cooper, 2026).
Many people have life insurance policies. However, a suicide clause is a standard clause in life insurance policies that limits payments made to survivors of a policyholder who dies by suicide within a certain period after purchasing the policy. Insurance companies typically do not pay a death benefit if the covered person dies by suicide within the first two years of coverage, commonly known as the exclusion period.
When the exclusion period ends, the policy’s beneficiaries can receive a death benefit if the covered person dies by suicide (Insuranceopedia, 2024).
POSTVENTION SERVICES AVAILABLE IN WASHINGTON STATE
Programs are available throughout Washington State to support people who have lost a loved one to suicide, such as Washington Support after Suicide (formerly known as CC Cares), offered by Crisis Connections. This program serves those newly bereaved by suicide. It was originally started and nurtured by Forefront Suicide Prevention at the University of Washington (Crisis Connections, 2026).
The Washington State Department of Health also lists many grief support resources on its website, such as the Healing Conversations Program for survivors of suicide loss. (See also “Resources” at the end of this course.)
POSTVENTION SUPPORT TO MILITARY FAMILIES
Military-sponsored programs for families and next of kin have been established to assist military dependents. Most commonly, a casualty assistance office works with them. Mental health and counseling services are available to all dependents, as are religious, financial, and legal services. A military family life consultant is available to work with the families.
- Casualty Assistance Program provides support for understanding all benefits and other forms of assistance.
- Veterans Affairs Bereavement Counseling offers bereavement support to parents, spouses, and children of active-duty and Guard or Reserve members who died while on military duty.
- Tragedy Assistant Program for Survivors (TAPS) is a national nonprofit veteran’s service organization that provides services to help stabilize family members in the immediate aftermath of a suicide.
- TRICARE provides mental health care services during bereavement; outpatient psychotherapy is covered for up to two sessions per week in a combination of individual, family, group, or collateral sessions.
- Bereavement camps and other groups for children include:
- Comfort Zone Camp
- The Dougy Center
- Eluna
- Good Grief Camps
- SnowballExpress
(TAPS, 2026; Military One Source, 2026)
ETHICAL ISSUES AND SUICIDE
Healthcare providers are guided by a code of ethics based on the principles of:
- Autonomy: Respect for the individual’s self-determination
- Beneficence: Doing the greatest possible good
- Nonmaleficence: Preventing or minimizing harm
- Justice: Fairness and equal access to care
Suicide prevention may involve ethical dilemmas. Emergent intervention may include:
- Actions taken without the individual’s consent
- Actions that limit a person’s freedom
- Actions that often feel and are disempowering
These challenge ethical imperatives, including:
- The right of a person to autonomous choice versus the need to protect vulnerable people (do no harm)
- Confidentiality versus the release or solicitation of information in order to prevent harm
- Freedom of choice to decide to live or die versus everything necessary should be done to preserve life
Involuntary hospitalizations and compulsory treatment can raise legal and ethical issues, as they violate basic civil rights, restrict the freedom of individuals, and impose significant responsibilities on physicians. This high sense of responsibility may cause physicians to cross their limits and ignore the autonomy of individuals while exercising their authority.
Healthcare providers’ duty to do no harm (nonmaleficence) can contradict the autonomy of a patient with suicidal ideation. Reporting suicide ideation to members of the healthcare team not providing direct care to a patient complies with the beneficence principle; however, this would breach patient confidentiality. This leads to a dilemma; neither can be chosen without violating the other.
The ethical principle of autonomy calls for respect, dignity, and choice, and therefore a person should not be coerced or manipulated into treatment if they are capable of autonomous decision-making. Taking away a person’s freedom when no crime has been committed is a very serious enterprise. Cases involving a patient who is experiencing suicidal thoughts and behaviors are classic examples of what is considered justified involuntary hospitalization. However, there is ambivalence concerning this, and it is argued by some that the risk of suicide by itself may not be sufficient justification and can increase the risk of suicide following discharge.
Evidence is accumulating about harms inherent in civil commitment. These arguments include:
- Inadequate attention has been given to the harms resulting from the use of coercion and the loss of autonomy.
- Inadequate evidence exists that involuntary hospitalization is an effective method to reduce deaths by suicide.
- Some patients with suicidal ideation may benefit more from therapeutic interventions that maximize and support autonomy and personal responsibility.
(Congress.gov, 2023; Laureano et al., 2024; Lee, 2025)
Differing Perspectives
There are several different perspectives when approaching the question of what should be done about a patient who has expressed verbally or by action the wish to die. Three such points of view are the libertarian, the communitarian, and the egalitarian-liberal perspectives.
The libertarian perspective is centered on the idea of autonomy and generally rejects involuntary hospitalization because it:
- Takes away the person’s freedom
- Restricts what the person can do with their body
- Prevents the person from protecting property (job, home)
- Is a means to manage people who do not adhere to social norms
- Coerces and manipulates patients into treatment
- Raises financial issues that may affect the patient or infringe on the property rights of other citizens (e.g., use of tax dollars)
- Does not recognize that suicide is sometimes a rational choice based on competent thought and decision-making skills
The communitarian perspective disregards the person’s autonomy and exclusively considers the community values of the clinician making the decision. It views suicide as morally wrong and offensive to the dominant group, and intervention must take place to prevent it.
The egalitarian-liberal perspective emphasizes the equality of access to resources. This approach states that the government’s role is to protect individual rights and that the right to health is a priority. If the right to health is not protected, then the rights of liberty and autonomy may not be possible. Involuntary hospitalization protects the person from a decision-impairing disease or disorder that puts the patient at risk for self-injury or death, and treatment of said disease or disorder gives the patient the right of health. However, the question remains as to how a mental health professional can know in advance that forcible treatment is justified, especially since there are no objective tests to verify whether or not a decision-impairing disease or disorder may or may not exist (Sandu et al., 2018).
CONCLUSION
Suicide—the deliberate ending of one’s own life—is an important public health concern around the world. Many complex factors contribute to a person’s decision to die by suicide, including biologic, psycho-sociocultural elements, and adverse life events. One important thing to consider is that most people are ambivalent about dying by suicide. They are caught in a situation from which they see no way out but to end their lives. This ambivalence is important, as it is the starting point at which an effective intervention can occur.
It is imperative that healthcare professionals understand the ways in which they can assess and manage individuals who are experiencing suicidal behaviors and learn the skills necessary to effectively intervene and prevent a suicide from happening. These skills include:
- Recognizing who is at risk, especially those who may be at high risk in the near future
- Learning how to communicate openly with those suspected to be at risk
- Responding to the needs of persons who have attempted suicide and survived in order to prevent future suicidal behavior
- Working with survivors of a suicide loss to help protect them from consequences such as taking their own lives, PTSD, and depression
- Providing suicide prevention education to others
RESOURCES
Ask Suicide-Screening Questions (ASQ)
Columbia-Suicide Severity Rating Scale (C-SSRS)
National Strategy for Suicide Prevention (National Action Alliance for Suicide Prevention)
Suicide & Crisis Lifeline
988 (call or text)
800-273-TALK (8255)
Suicide Data and Statistics (CDC)
Suicide Prevention (National Institute of Mental Health)
Suicide Prevention Resource for Action (CDC)
Suicide Prevention Resources (CDC)
Washington State
Forefront Suicide Prevention (University of Washington)
Grief Support and Resources (WA State DOH)
Safe Medication Return (WA State DOH)
Suicide Prevention (WA State DOH)
Washington resources (Suicide Prevention Resource Center)
Washington Suicide Hotlines (Suicide.org)
REFERENCES
Aamar R. (2025). Suicide risk assessment: How to talk about suicidal ideation. Relias. https://www.relias.com/blog/suicide-risk-assessment
American Academy of Pediatrics (AAP). (2023). Screening for suicide risk in clinical practice. https://www.aap.org/en/patient-care/blueprint-for-youth-suicide-prevention/strategies-for-clinical-settings-for-youth-suicide-prevention/screening-for-suicide-risk-in-clinical-practice/
American Foundation for Suicide Prevention (AFSP). (2026a). Ethical reporting guidelines for media. https://afsp.org/ethicalreporting/#guidelines-for-ethically-reporting-on-suicide
American Foundation for Suicide Prevention (AFSP). (2026c). Risk factors, protective factors and warning signs. https://afsp.org/risk-factors-protective-factors-and-warning-signs
American Foundation for Suicide Prevention (AFSP). (2026e). Therapies. https://afsp.org/therapies
American Psychiatric Association (APA). (2013). Diagnostic and statistical manual of mental disorders (5th ed.).
American Psychological Association (APA). (2026). APA dictionary of psychology. https://dictionary.apa.org/mass-suicide
American Psychological Association (APA). (2025). Trauma before enlistment linked to high suicide rates among military personnel, veterans. https://www.socialworktoday.com/news/dn_081314.shtml
Association for Behavioral and Cognitive Therapies (ABCT). (2025). Military suicide. https://www.abct.org/fact-sheets/military-suicide
Avery S. (2022). Four genes identified as heightening risk of suicidal thoughts/actions. https://psychiatry.duke.edu/news/four-genes-identified-heightening-risk-suicidal-thoughtsactions
Bateson J. (2025). Is there a link between economic factors and suicide? Psychology Today. https://www.psychologytoday.com/us/blog/goodbye-suicide/202510/is-there-a-link-between-economic-factors-and-suicide
Bommersbach T, Rosenheck R, & Rhee T. (2022). National trends of mental health care among US adults who attempted suicide in the past 12 months. JAMA Psychiatry, 79(3), 219–231. https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2787969
California Evidence-Based Clearinghouse for Child Welfare (CEBC). (2026). Suicide behaviors questionnaire–revised (SBQ-R). https://www.cebc4cw.org/assessment-tool/suicide-behaviors-questionnaire-revised
Caregiving in the US. (2025). Caregiving in the US research report. https://www.caregivingintheus.org/app/uploads/2026/02/Final-2025-CGUS-Report-1.pdf
Centers for Disease Control and Prevention (CDC). (2026). Suicide and occupation. https://www.cdc.gov/niosh/stress/suicide/?CDC_AAref_Val=https://www.cdc.gov/niosh/topics/stress/suicide.html
Centers for Disease Control and Prevention (CDC). (2025c). Suicide rates by state. https://www.cdc.gov/suicide/facts/rates-by-state.html
Centers for Disease Control and Prevention (CDC). (2024a). Bullying victimization among teenagers: United States, July 2021–December 2023. https://www.cdc.gov/nchs/products/databriefs/db514.htm
Centers for Disease Control and Prevention (CDC). (2024b). Health disparities in suicide. https://www.cdc.gov/suicide/disparities/index.html
Centers for Disease Control and Prevention (CDC). (2024c). Preventing suicide. https://www.cdc.gov/suicide/prevention/index.html
Centers for Disease Control and Prevention (CDC). (2024d). Risk and protective factors for suicide. https://www.cdc.gov/suicide/factors/index.html
Children’s Hospital Association (CHA), Pediatric Health Information System (PHIS). (2025). Addressing pediatric suicide. https://www.childrenshospitals.org/content/behavioral-health/summary/the-state-of-pediatric-suicide
Chiles J, Strohasi K, & Roberts L. (2024). Clinical manual for assessment and treatment of suicidal patients (2nd ed.). American Psychiatric Association Publishing.
Columbia University. (2021). A simple set of 6 questions to screen for suicide. https://www.columbiapsychiatry.org/news/simple-set-6-questions-screen-suicide
Congress.gov. (2023). Involuntary civil commitment: Fourteenth amendment due process protections. https://www.congress.gov/crs-product/R47571
Cooper A. (2026). Does health insurance cover when injuries is self inflicted? Insurance Informant. https://insuranceinformant.com/does-health-insurance-cover-when-injuries-is-self.html
Crisis Connections. (2026). Washington support after suicide. https://www.crisisconnections.org/wasas/
Dean J. (2025). The alternative lifestyles linked to suicide and self-harm. Psyblog. https://www.spring.org.uk/2025/01/alternative-lifestyles-suicide.php
Desai R, Tsipa A, Fearn C, et al. (2024). Suicide and dementia: A systematic review of meta-analysis of prevalence and risk factors. Ageing Research Reviews, 100, 102445. https://www.sciencedirect.com/science/article/pii/S1568163724002630
Discovery Mood & Anxiety Program. (2025). The difference between self-harm and attempted suicide. https://discoverymood.com/blog/difference-self-harm-attempted-suicide/
Dwivdei Y, Roy B, & Korla P. (2025). Genome-wide methylome-based molecular pathologies associated with depression and suicide. Neuropsychopharmacology, 50, 705–16. https://www.nature.com/articles/s41386-024-02040-9
Education Development Center (EDC). (2026). Least restrictive care. https://zerosuicide.edc.org/toolkit/treat/least-restrictive-care
Gorn D. (2026). Veterans in America. RAND Corporation. https://www.rand.org/multimedia/podcasts/veterans-in-america/why-so-many-military-women-think-about-suicide.html
Grieve R. (2023). Chapter 3: Basic attending and listening skills. http://people.wku.edu/rick.grieve/Clinical%20Interviewing/pp/ChapterThree.pdf
Harvard T. H. Chan School of Public Health (HSPH). (2023). Suicide, guns, and public health. https://hsph.harvard.edu/research/means-matter/
Hawgood J, Woodward A, Quinnett P, et al. (2022). Gatekeeper training and minimum standards of competency: Essentials for the suicide prevention workforce. Crisis: The Journal of Crisis Intervention and Suicide Prevention, 43(6), 516–22.
Hu X, Zhang A, Wang C, & Zhang X. (2025). Melatonin rhythm disorder is more pronounced in major depressive disorder with non-suicidal self-injury. Frontiers in Neuroscience, 19, 1534715. https://www.frontiersin.org/journals/neuroscience/articles/10.3389/fnins.2025.1534715/full
Insuranceopedia. (2024). Suicide clause. https://www.insuranceopedia.com/definition/4419/suicide-clause
The Jed Foundation. (2023). Youth suicide: Current trends and the path to prevention. https://jedfoundation.org/wp-content/uploads/2024/06/JED-Suicide-Trends-Report_June-2024.pdf
Jobes D. (2026). Cultural perspectives on suicide: How different societies approach prevention. CAMS.care. https://cams-care.com/resources/blog/cultural-perspectives-on-suicide-how-different-societies-approach-prevention/
The Joint Commission (TJC). (2026). Suicide prevention. https://www.jointcommission.org/resources/patient-safety-topics/suicide-prevention/
Kennebeck S & Bonin L. (2025). Suicidal behavior in children and adolescents: Epidemiology and risk factors. UpToDate. https://www.uptodate.com/contents/suicidal-behavior-in-children-and-adolescents-epidemiology-and-risk-factors
Laureano CD, Laranjeira C, Querido A, et al. (2024). Ethical issues in clinical decision-making about involuntary psychiatric treatment: A scoping review. Healthcare (Basel), 12(4), 445. https://pmc.ncbi.nlm.nih.gov/articles/PMC10888148/
Lee S. (2025). The bioethics of involuntary commitment. NumberAnalytics. https://www.numberanalytics.com/blog/bioethics-involuntary-commitment
Levin M, Jury N, Mohseni K, et al. (2026). Do antidepressants increase suicide attempts? Do they have other risks? https://www.center4research.org/antidepressants-increase-suicide-attempts-risks/
Mayo Clinic. (2024). Self-injury/cutting. https://www.mayoclinic.org/diseases-conditions/self-injury/symptoms-causes/syc-20350950
Mejia MC, Hennekens CH, Levine RS, et al. (2024). Deaths of despair: A major and increasing contributor to United States deaths. Advances in Preventative Medicine and Health Care, 7, 1062. https://www.gavinpublishers.com/assets/articles_pdf/Deaths-of-Despair-A-Major-and-Increasing-Contributor-to-United-States-Deaths.pdf
Military One Source. (2026). Casualty assistance: Resources. https://www.militaryonesource.mil/casualty-mortuary-affairs/casualty-assistance/resources/
Miron O, Yu KH, Wilf-Miron R, et al. (2019). Suicide rates among adolescents and young adults in the United States, 2000-2017. JAMA, 321(23), 2362–2364. https://jamanetwork.com/journals/jama/fullarticle/2735809
Moutier C. (2026). Suicidal behavior. Merck Manual. https://www.merckmanuals.com/professional/psychiatric-disorders/suicidal-behavior-and-self-injury/suicidal-behavior
National Action Alliance for Suicide Prevention (NAASP), Lethal Means Stakeholder Group. (2020). Lethal means and suicide prevention: A guide for community and industry leaders. https://theactionalliance.org/resource/lethal-means-suicide-prevention-guide-community-industry-leaders
National Council on Aging (NCOA). (2025). Suicide and older adults: What you should know. https://ncoa.org/article/suicide-and-older-adults-what-you-should-know
National Institute of Mental Health (NIMH). (2026). Ask suicide-screening questions (ASQ) toolkit. https://www.nimh.nih.gov/research/research-conducted-at-nimh/asq-toolkit-materials
Norful A. (2025). A hidden crisis: Nurse suicide in America. Becker’s Clinical Leadership. https://www.beckershospitalreview.com/quality/nursing/a-hidden-crisis-nurse-suicide-in-america/
O’Rourke M, Jamil R, & Siddiqui W. (2023). Suicide screening and prevention. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK531453/
PsychDB. (2025). Suicide risk assessment (SRA). https://www.psychdb.com/teaching/suicide-risk-assessment-sra
Purdue University. (2025). QPR suicide prevention gatekeeper training available this fall. https://www.purdue.edu/caps/support/outreach/qpr-mhfa.php
Sandu A, Frunza A, Lliescu A, et al. (2018). A metaethical perspective on non-voluntary psychiatric hospitalization. Arch euromedica, 8(1), 117–20.
Schreiber J & Culpepper L. (2025). Suicidal ideation and behavior in adults. UpToDate. https://www.uptodate.com/contents/suicidal-ideation-and-behavior-in-adults
Sharma P. (2024). 8 common myths about suicide. Mayo Clinic Health Systems. https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/8-common-myths-about-suicide
Sinyor M, Silverman M, Pirkis J, et al. (2024). The effect of economic downturn, financial hardship, unemployment, and relevant government responses on suicide. The Lancet, 9(10), E802–E806. https://www.thelancet.com/journals/lanpub/article/PIIS2468-2667%2824%2900152-X/fulltext
Smith A. (2025). These factors could be behind the military’s shockingly high suicide rates. Science Alert. https://www.sciencealert.com/these-factors-could-be-behind-the-militarys-shockingly-high-suicide-rates
Sommers-Flanagan J. (2024). Working with emotions in counseling and psychotherapy: Part 2. https://johnsommersflanagan.com/2024/03/19/working-with-emotions-in-counseling-and-psychotherapy-part-2/
Sommers-Flanagan J. (2022). Suicide assessment for clinicians: A strengths-based model. https://www.continuingedcourses.net/active/courses/course114.php
Soreff S. (2026). Suicide. Medscape. https://emedicine.medscape.com/article/2013085-overview#a4
Sruthi M. (2025). What age group is the most suicidal? MedicineNet. https://www.medicinenet.com/what_age_group_is_the_most_suicidal/article.htm
Suicide Prevention Alliance. (2026). Suicide language. https://www.suicidepreventionalliance.org/about-suicide/suicide-language/
Suicide Prevention Resource Center (SPRC). (2025a). A comprehensive approach to suicide prevention. https://sprc.org/effective-prevention/comprehensive-approach
Suicide Prevention Resource Center (SPRC). (2025b). Provide for immediate and long-term postvention. https://sprc.org/effective-prevention/a-comprehensive-approach-to-suicide-prevention/provide-for-immediate-and-long-term-postvention/
Suicide Prevention Resource Center (SPRC). (2025c). Reduce access to means of suicide. https://sprc.org/effective-prevention/a-comprehensive-approach-to-suicide-prevention/reduce-access-to-means-of-suicide/
Tera D. (2025). Life cycle and suicidal behavior among women: Why midlife matters. Mindful Path. https://www.mindfulpathpsy.org/post/life-cycle-and-suicidal-behavior-among-women-why-midlife-matters
Tragedy Assistance Program for Survivors (TAPS). (2026). Caring for the families of America’s fallen heroes. https://www.taps.org/
U.S. Department of Veterans Affairs (VA). (2025). The relationships between PTSD and suicide. https://www.ptsd.va.gov/professional/treat/cooccurring/suicide_ptsd.asp
U.S. Department of Veterans Affairs (VA). (2024). VA/DoD clinical practice guidelines. https://www.healthquality.va.gov/guidelines/mh/srb/
U.S. Department of Veterans Affairs (VA). (2023). Office of public and intergovernmental affairs. https://www.va.gov/opa/pressrel/pressrelease.cfm?id=5852
U.S. Department of Veterans Affairs (VA). (2018). National strategy for preventing veteran suicide 2018–2028. https://www.mentalhealth.va.gov
U.S. Preventive Services Task Force (USPSTF). (2023). Depression and suicide risk in adults: Screening. https://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/suicide-risk-in-adolescents-adults-and-older-adults-screening
Van Orden K. (2023). Suicide risk in caregivers. International Psychogeriatrics, 35(12), 695–7. https://www.intpsychogeriatrics.org/article/S1041-6102(24)03010-2/fulltext
Washington State Department of Health (WSDOH). (2025a). 2024 death with dignity act report. https://doh.wa.gov/sites/default/files/2026-02/422-109-DeathWithDignityAct2024.pdf
Washington State Department of Health (WSDOH). (2025b). 2025 Washington State suicide prevention plan. https://doh.wa.gov/sites/default/files/2025-05/971076-SuicidePreventionPlan.pdf
Washington State Legislature. (n.d.). Chapter 71.05 RCW, behavioral health disorders. https://app.leg.wa.gov/rcw/default.aspx?cite=71.05
Werne M. (2024). Tough topic: Suicide assessment and prevention. CAMFT. https://www.camft.org/Membership/About-Us/Pre-licensee-E-news/Winter-2024-Pre-Licensed-E-Newsletter/Tough-Topic-Suicide
Wiedemann A, Jones P, & Burn A. (2024). Impact of the COVID-19 pandemic on young adults’ mental health and beyond: A qualitative investigation nested with an ongoing general population cohort study. Social Psychiatry and Psychiatric Epidemiology, 59(12), 2203–13. https://pmc.ncbi.nlm.nih.gov/articles/PMC11522157
Wikiversity. (2023). Evidence-based assessment/Rx4DxTx of self-harm. https://en.wikiversity.org/wiki/Evidence-based_assessment/Rx4DxTx_of_self_harm#Assessment_Table_for_Suicidality_and_NSSI
Wislowska-Stanek A, Kolosowska K, & Maciejak P. (2021). Neurobiological basis of increased risk for suicidal behavior. Cells, 10(10), 2519. https://doi.org/10.3390/cells10102519
Wrench J, Punyanunt-Carter N, & Thweatt K. (2026). Listening responses. LibreTexts. https://socialsci.libretexts.org/Bookshelves/Communication/Interpersonal_Communication/Interpersonal_Communication_-_A_Mindful_Approach_to_Relationships_(Wrench_et_al.)/07%3A_Talking_and_Listening/7.04%3A_Listening_Responses
Young E, McCain J, Mercado M, et al. (2024). Frequent social media use and experiences with bullying victimization, persistent feelings of sadness or hopelessness, and suicide risk among high school students—Youth risk behavior survey, United States, 2023. MMWR, 73(4), 23–30.
Customer Rating
4.9 / 146 ratings